30% present as emergencies (obstruction/strangulation)
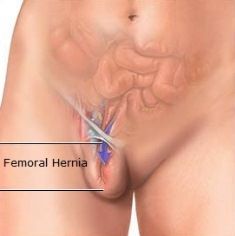
Found infero-lateral to the pubic tubercle – but if it rolls upwards over the inguinal ligament can be mistaken for an inguinal
Differential diagnoses: inguinal hernia, femoral canal lipoma or lymph node, saphena varix (dissapears on lying and has palpable thrill on coughing), femoral artery aneurysm
Risk of strangulation: 22% after 3 months, 45% after 21 months.
Surgical Technique
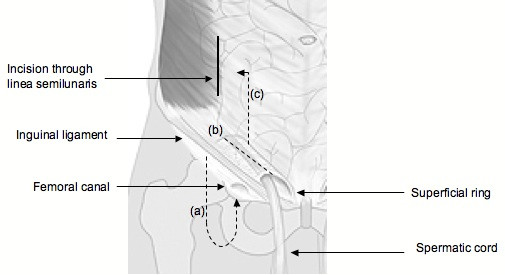
Modified McEvedy’s:
- A skin incision is made 1cm above the medial aspect of the inguinal ligament.
- If a femoral hernia is confirmed, it can be approached from below the inguinal ligament (a)
- If entry to the abdomen is required, go 4cm above the inguinal ligament and divide the linea semilunaris (anterior rectus sheath) vertically and retract the rectus muscle medially.(c)
- If an inguinal hernia is found, the canal can be entered by splitting the external oblique (b)
5. If the lacunar ligament needs to be divided, be aware that 10% will have an abnormal obturator artery at its cresenteric margin