Endoscopic Mucosal Resection
Used for resection of superficial neoplasms
Basic principles are demarcation of the lesion, submucosal injection to lift the lesion and endoscopic snare resection.
Paris classification:
developed by the Japanese Society of Gastrointestinal Endoscopists JSGE in 2002 –
(All are) Superficial = 0
Type 0-I = polypoid
Type 0-II = non-polypoid
0-Ip = polypoid, pedunculated
0-Is = polypoid, sessile
0-IIa = sessile, slightly elevated
0-IIb = sessile, flat
0-IIc = sessile, slightly depreseed
0-III = excavated
Vienna Classification
Non-invasive (low-grade, high-grade)
Invasive (intramucosal cancer, cancer infiltrating submucosa)
EUS produces an image with 9 distinct layers to the mucosal wall. The depth of invasion determines the likelihood of LN involvement.
Accuracy of EUS: 77% for TI disesase
90% for T4 disease
75% for LN involvement
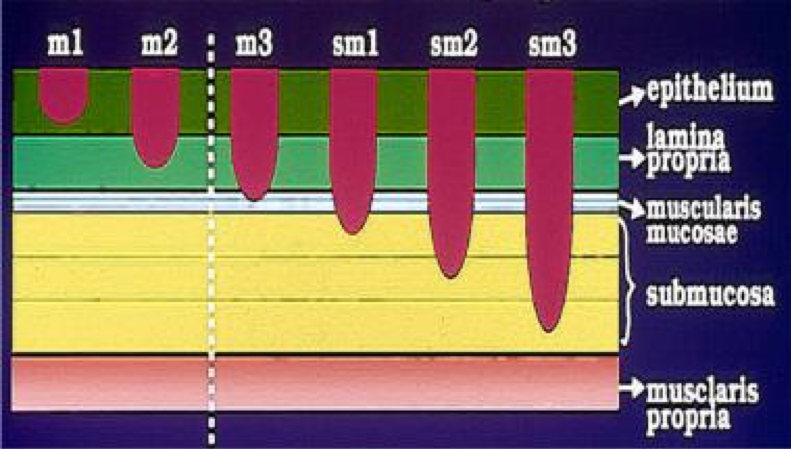
Schematic of penetration as determined by histology
False-positive EUS images can be due to peritumour inflammation
False-negative due to to micrometastases (upto 44%)
Indications
1. Definitive treatment of superficial pre-malignant and well-to-moderately differentiated malignancies when there are no LN or distant metastases.
2. As part of the staging for early GI cancer
SCC of oesophagus: JSGE guidelines advice lesions less than 2cm long and covering less than 1/3rd circumference
Barrett’s: For irregularities including nodularity or ulceration. IF the specimen confirms definitive resection of cancer or only high-grade dysplasia, then ablative therapy should be given. If however, It shows cancer invading the margin (particularly deep margin), either surgery or systemic therapy should be considered.
Early gastric cancer:
NB. JSGE states that well to moderately differentiated tubular and papillary adenocarcinomas are differentiated carcinomas whereas signet ring cell and poorly differentiated are undifferentiated.
Decision to EMR depends on the size of the lesion, the depth of invasion, presence of ulceration and whether its differentiated or undifferentiated.
Absolute indications: lesions that are intramucosal and less than 2cm, whilst macroscopic type doesn’t matter there shouldn’t be any ulceration (UL-)
Extended indications:
– UL- T1a differentiated cancers >2cm
– UL+ T1a differentiated cancers <3cm
– UL- T1a undifferentiated cancers <2cm
HOWEVER, for these extended indications, the JSGE recommends ESD (endoscopic submucosal dissection), because a retrospective Japanese study showed that R0 margins are achieved more with ESD in these cases. There are no randomised studies.
In the UK, standard treatment for extended indications would be surgery.
Duodenal lesions:
EMR can be used to resect or stage ampullary/periampullary adenomas, early carcinomas, ampullary submucosal lesions.
Additional indications can be neuroendocrine tumours.
However, they are associated with substantial rates of complications.
Colonic lesions
(not detailed)
Mark Henwood’s oesophagus EMR 07/01/2019
Define the distal extent of the lesion, inject mix (gelofusin, adrenaline 1:1000, indigo blue) into the edges to lift, place snare around it and cut
The edges looked to be nodular still afterwards and some of the lesion seemed to be left behind but these couldn’t be lifted to get a snare on, so were left behind.
Mark Henwood’s gastric EMR 07/01/2019
Ulcerated lesion on lesser curve.
Using cap assisted (rubber band ligation) he took it in pieces – placing rubber bands to lift, cutting with snare and then retrieving using the suction, one piece at a time until all of it was removed. Again, edges looked nodular.