Gastric Cancer
‘Suspicious’ gastric ulcers should be re-biopsied at the edge in a ‘drill’ manner whereby deeper biopsies are taken through the same spot.
If the histology is poorly differentiated, it wouldn’t be suitable for EMR. (<2cm, well/mod differentiated, not ulcerated). With gastric cancers, even if there is submucosal and LN involvement, the 5-year survival is much better than with advanced disease (compare with with oesophageal, where submucosal involvement has dire outcomes)
IF the lesion is more than 5cm from the GOJ, the operation of choice would be a subtotal gastrectomy.
Staging for gastric cancer:
CT chest/abdo/pelvis
Laparoscopy
T
· T1
o T1a: tumour invades the lamina propria and or muscularis mucosae
o T1b: tumour invades submucosa
· T2: tumour invades muscularis propria
· T3: tumour penetrates the serosa without invasion of the adjacent structures
· T4
o T4a: tumour invades serosa (visceral peritoneum)
o T4b: tumour invades adjacent structures
N
· N0: no nodal involvement
· N1: metastases in 1 to 2 regional lymph nodes
· N2: metastases in 3 to 6 regional lymph nodes
· N3
o N3a: metastases in 7 to 15 regional lymph nodes
o N3b: metastases in more than 15 regional lymph nodes
M
· M0: no distant metastases
· M1: distant metastases
How to do a subtotal gastrectomy
Midline incision
Examine abdomen
Open the plane between the omentum and transverse mesocolon
Lead down to the right gastro-epiploic vessels which can be ligated and divided.
Open the gastrohepatic ligament and identify right gastric vessel. Ligate and divide.
Create a plane behind D1, separating off the pancreas. Divide with TLC and oversaw the staple line.
Divide posterior gastric attachments to pancreas. Identify the left gastric vessels and divide.
Identify point for division on greater curve – normally just below the first short gastric. Divide to the lesser curve with TLC.
Bring roux limb through transverse mesocolon and anastomose with 2-layer hand-sawn anastomoses to the stomach
Attach biliary limb 50cm distal to the gastro-jejunostomy as a jejuno-jejunostomy, again 2-layer hand-sawn.
Leave a drain next to duodenal stump and anastomosis.
Ideally a minimum of 15 nodes to be resected for reliable staging
If there is nodal involvement, even with T1 disease, chemotherapy (ECX) would be of benefit.
Evidence for chemotherapy in curative setting?
The MAGIC/UK MRC trial set the standard for gastric and GOJ tumour chemotherapy in resectable disease.
Peri-operative chemo with Epirubicin, cisplatin and 5-Fluorouracil (ECF) increased 5-year survival from 23% to 36% than surgery alone.
Capecitabine (X) is the oral pro-drug for 5-Fluorouracil and is just as efficacious, and doesn’t need CVP therefore many centers use ECXregimen.
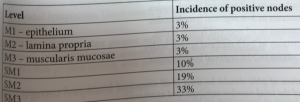
T-staging
Staging of mucosal and submucosa for gastric cancers
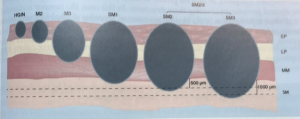
The T staging for gastric cancer is the same as for oesophageal cancer upto T2 – muscularis propria.
However, T3 in gastric cancer is tumour invading subserosal connective tissue WITHOUT invasion into visceral peritoneum
T4a – Tumour invading serosa (or visceral peritoneum)
T4b – tumour invades adjacent structures.
NB. A tumour can invade muscularis propria and then eneter gastrohepatic ligament or omentum, without perforating the visceral peritoneum lining these. These will be considered T3. Only if the visceral peritoneum is perforated, will it become T4.
Regional Lymph Nodes staging
NX Nodes cannot be assessed
N1 1-3 nodes positive
N2 3-6 nodes posititve
N3 ³7 nodes positive
N3a 7-15 nodes positive
N3b ³ 16 nodes positive