Surgical Nutrition
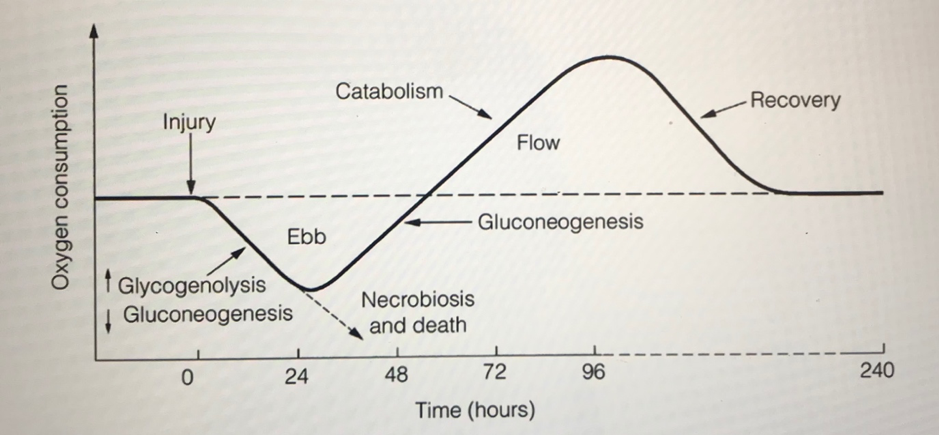
Sir David Cuthbertson described how response to injury could be considered in 2 phases:
1. The ‘ebb’ phase where there is a short-lived phase response associated with hypovalaemic shock (increased sympathetic activity and reduced metabolic rate)
a. Decraeased resting energy expenditure
b. Increased glyogenolysis
c. Decreased gluconeogenesis
2. The ‘flow’ phase where there is loss of body nitrogen and resultant negative nitrogen balance
a. Increased resting energy expenditure
b. Increased heat production, pyrexia
c. Increased muscle catabolism and wasting, loss of body nitrogen
d. Increased breakdown of fat and reduced fat synthesis
e. Increased gluconeogenesis and impaired glucose tolerance
If the ebb phase isn’t replaced by the flow phase, then despite any advances in surgery or anaesthesia, the patient will deteriorate and die.
The central nevous system pituitary origin hormones play a key role:
– Catecholamines: adrenalien and noradrenaline increase within a few minutes and return to normal within 24 hours
– Glucagon: rises to a maximal concentration 12-48 hours post-trauma
– Insulin: initially low and then rises to a maximum several days after injury
– Cortisol: rapid increase, normally returning to normal after 24-48 hours but can stay raised for several days
– Growth hormone: rises and returns to normal after 24 hours
– Thryroid hormones: after traum the ‘sick euthyroid syndrome’ can be present: TSH normal or low, T4 and T3 normal. These can last for several weeks
– Renin, aldosterone: renin made due to reduced renal perfusion, stimulating aldosterone
– Testosterone: plasma concentration falls after trauma and can remain low for 7 days
– Vasopressin/ADH: rises and can be raised for several days
– Cytokines: increased IL-2, IL-6, TNF etc