Laparoscopic Sleeve Gastrectomy
Originated as the first stage of the duodenal switch procedure.
Morceau et al modified Scopinaro’s procedure to have a longitudinal resection of the stomach to preserve the pylorus and increased the common channel length to 100cm, thereby performing the first LSG in 1999.
Data suggests that long-term weight loss is equal to RYGB, likely due to reduced Ghrelin from the resection of the fundus, alongside the decrease in capacity.
Sleeve capacity should be 100ml (10%) or less
Advantages:
· technically easier, shorter operative time, small bowel continuity maintained, pylorus preserved.
· Also, long-term nutritional problems avoided, complications such as internal hernias and SBO are avoided.
· Can later be converted to a RYGB/DS if necessary
Disadvantages:
· Long staple line and possibility of leak
· Can lead to chronic fistula
· Increased rate of reflux
Paper confirming long-term efficacy of weight loss:
Diamantis T et al. Review of long-term weight loss results after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2014;10(1):177-83
Contraindications:
Barrett’s oesophagitis
Long-standing T2DM
ASA IV
End-stage organ dysfunction
Malignancy
Cirrhosis with portal hypertension
Pre-operative workup
Detailed history:
– reflux symptoms, nature and frequency of each, medication being taken
– Chest pain, dyspnoea (may need cardiology review, echo, stress testing etc)
– Loud snoring or excessive day time sleepiness (may need respiratory review for OSA – pulse oximetry, ABG, PFTs, polysomnography. If they have OSA, should be on CPAP during sleep for at-least 5-7 days prior to surgery)
Perform OGD:
– extent of reflux oesophagitis, hiatal hernia, gastric/duodenal ulceration, H Pylori status
– Some may need 24hr pH studies, manometry and oesophageal biopsies to rule out Barrett’s
USS:
– Assess status of liver and rule out intra-abdominal pathology (high incidence of NASH)
Venous doppler both legs
– Rule out previous or existing DVTs
Preoperative dietician review for counselling about postoperative eating habits and choices
MDT: further tests may be needed to investigate for hidden co-morbidities
Pre-operative:
– Low calorie diet for 2 weeks
Equipment:
– Bariatric bed
– Foot boards
– Straps
– Long-instruments
– Self-retaining liver retractor (Nathanson – Cook Medical)
Preoperative antibiotics at induction eg Cefuroxime 2g iv.
Oro-gastric tube placed by anaesthetist
Positioning:
– Steep reverse Trendelenberg
– Split leg (French) position
– Flow-trons
– Secured to bed with straps, footboard and bandages
Intraoperative details
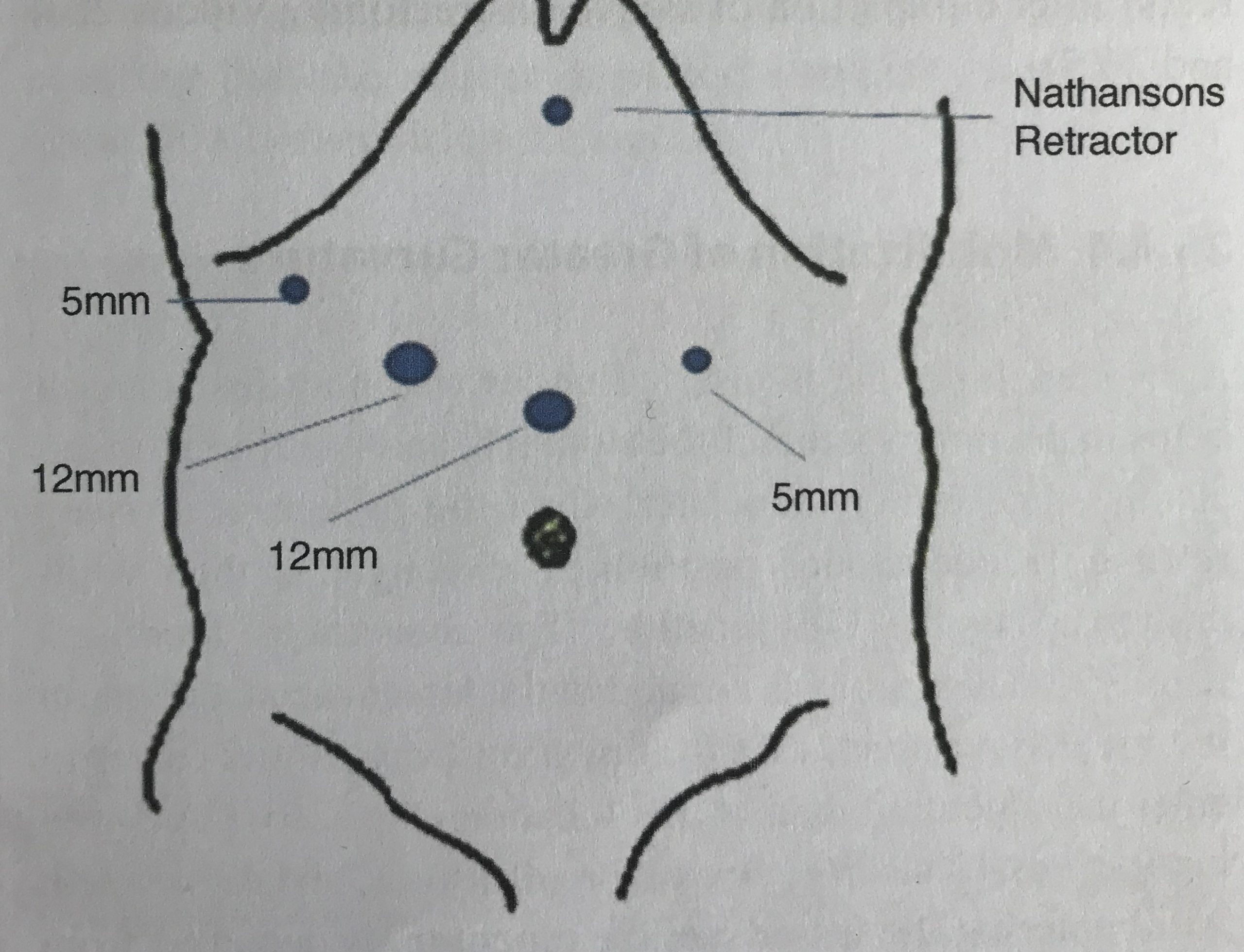
1. Ports:
a. Veress needle in supraumbilical region normally, but if previous operations then at Palmer’s point (2-fingers below subcostal margin at mid-clavicular line). Abdominal pressure between 15 and 20 mmHg
Or Optical entry with Visi-port Or Hassan technique in upper umbilicus
b. Normally, 2 x 12mm and 2 x 5mm ports are placed. (First 12mm port 15cm below xiphisternum for laparoscope 12mm working port in right mid-clavicular line; 5mm working port in right anterior axillary line, 5mm assistant port in left mid-clavicular line)
c. Placement of liver retractor in epigastrium.
d. Assess hiatus for laxity or hernia – if present, perform crural repair before commencing procedure.
{kind=link}
{kind=link}
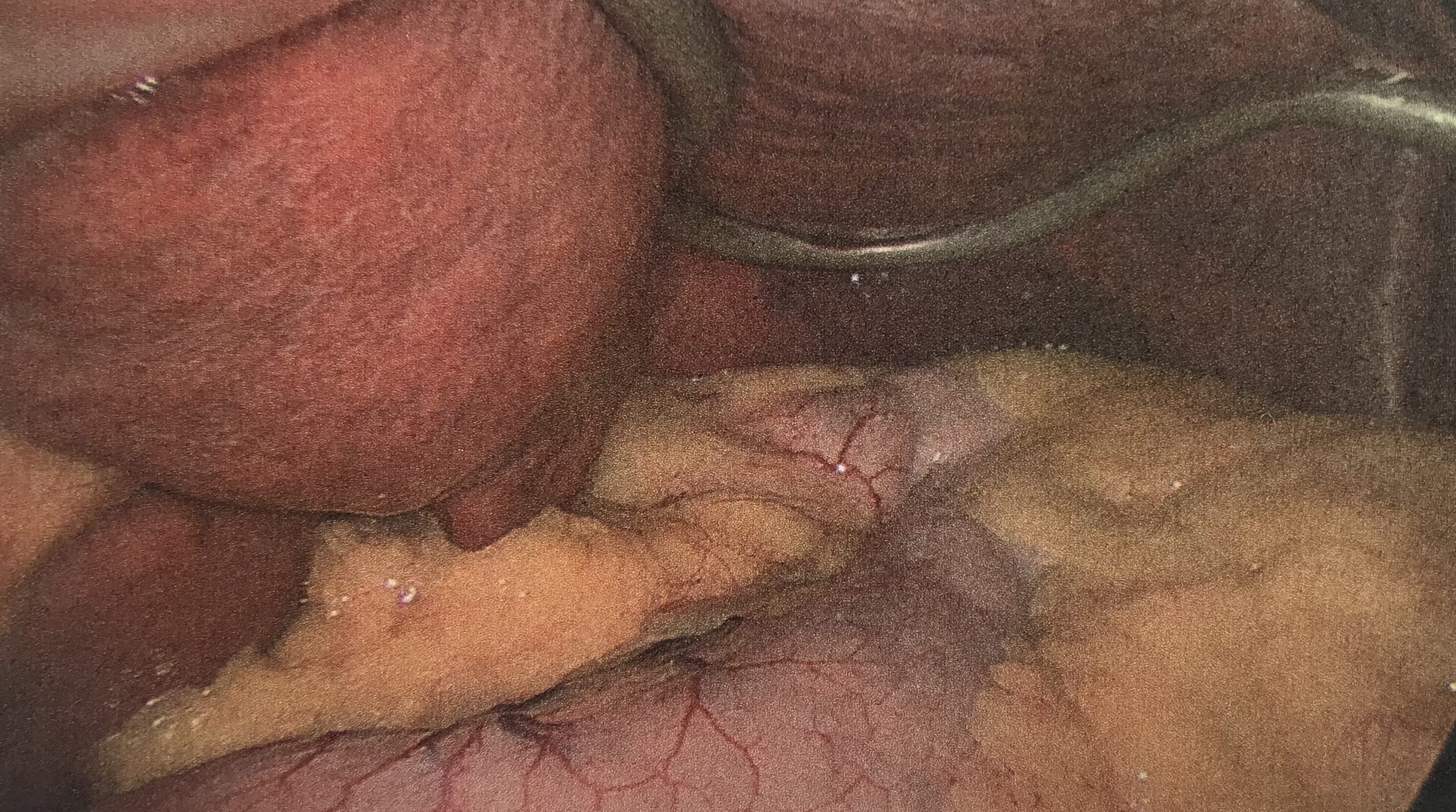
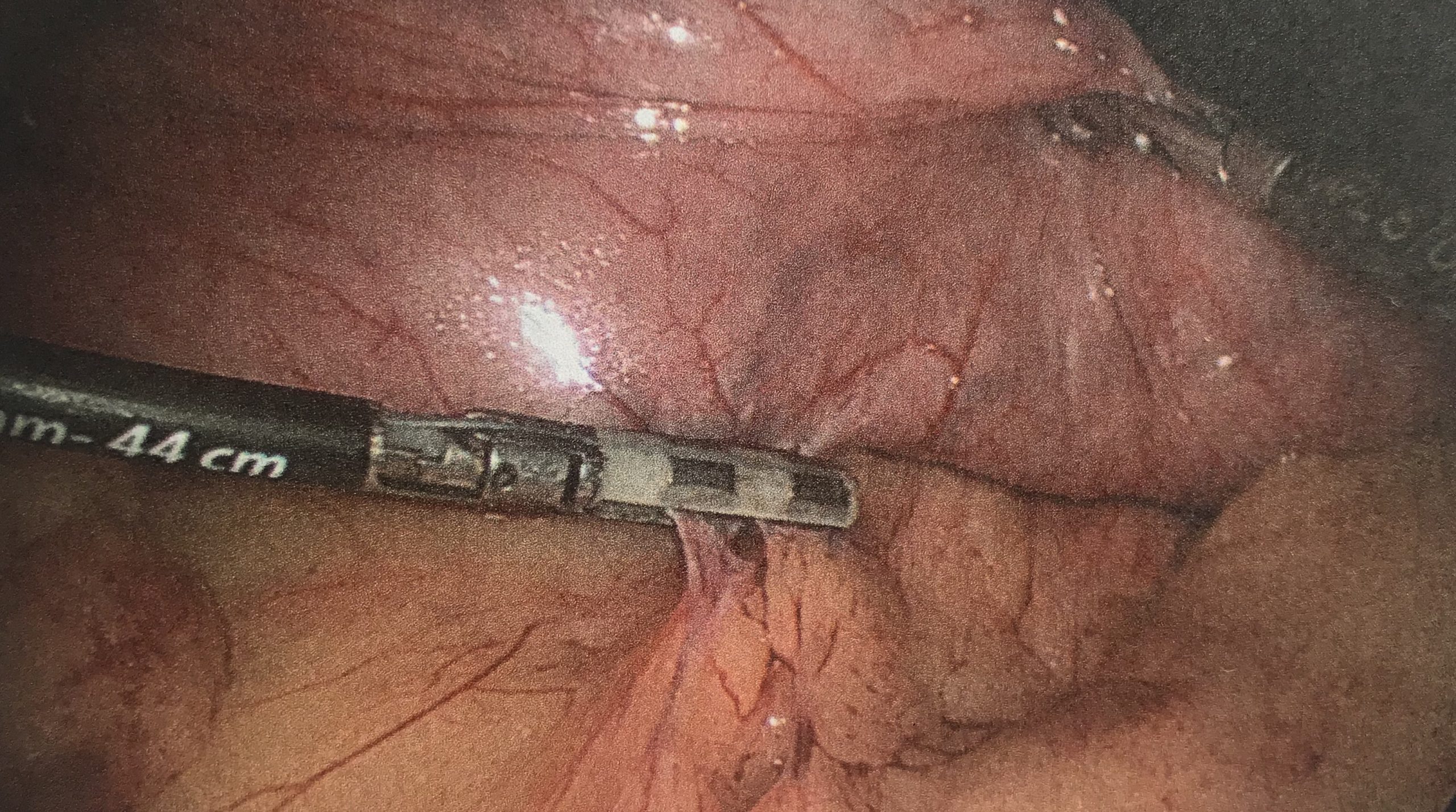
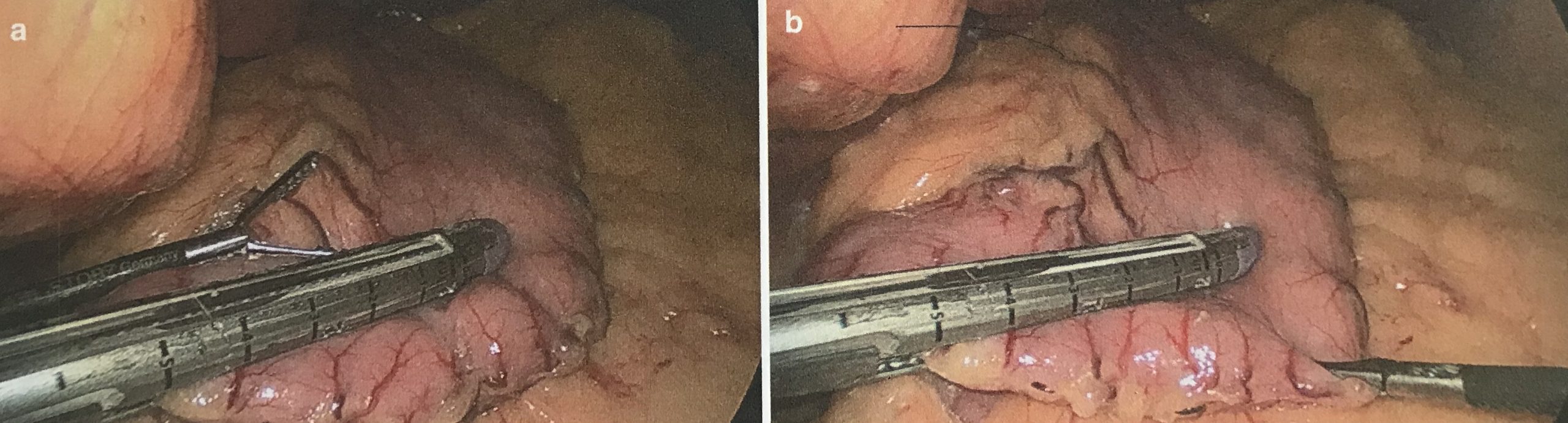
2. Mobilisation of greater curve
a. A 36-Fr bougie inserted which helps to decompress the stomach and then drawn upto the GE junction.
b. Incisura is identified
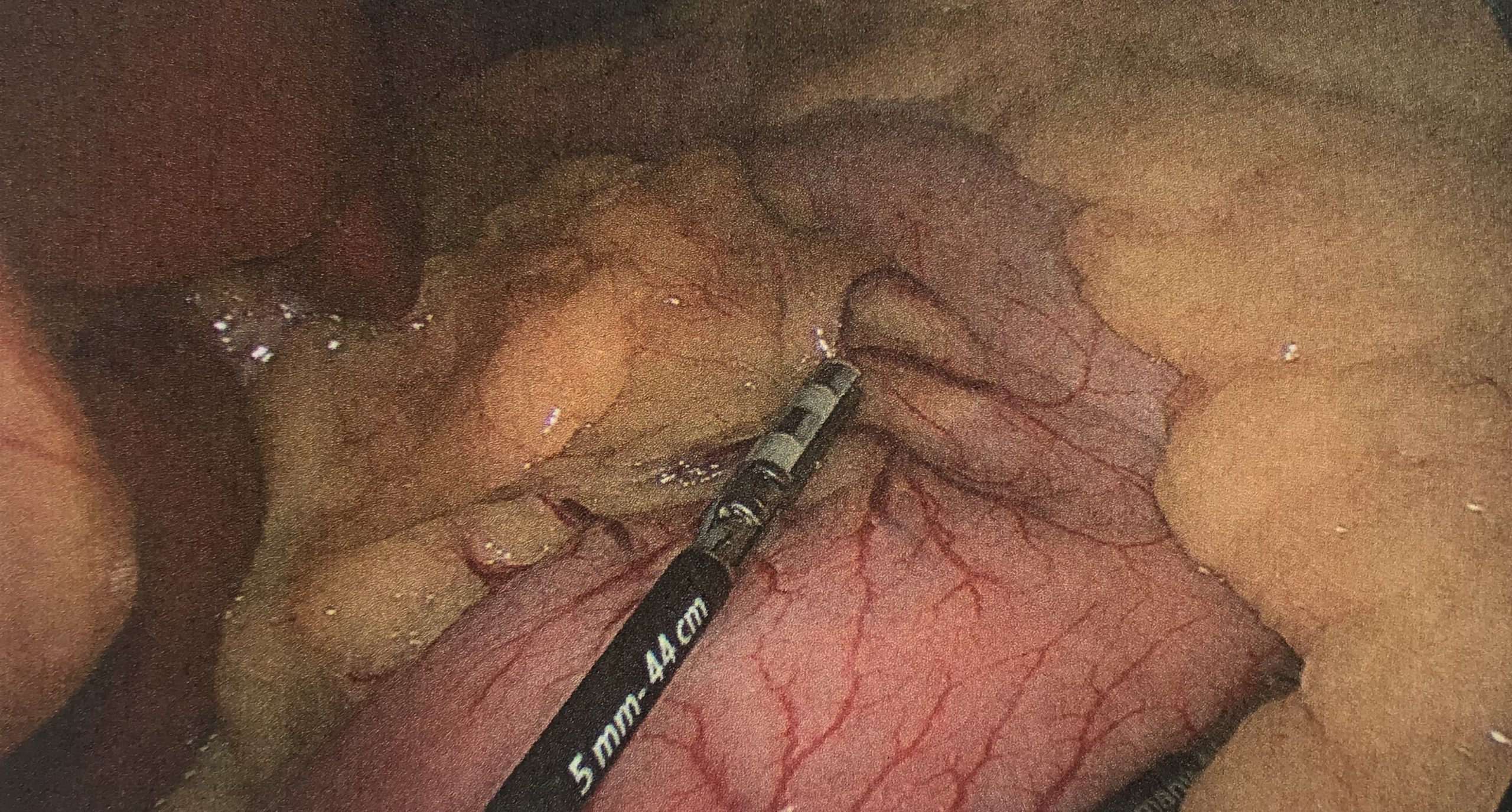
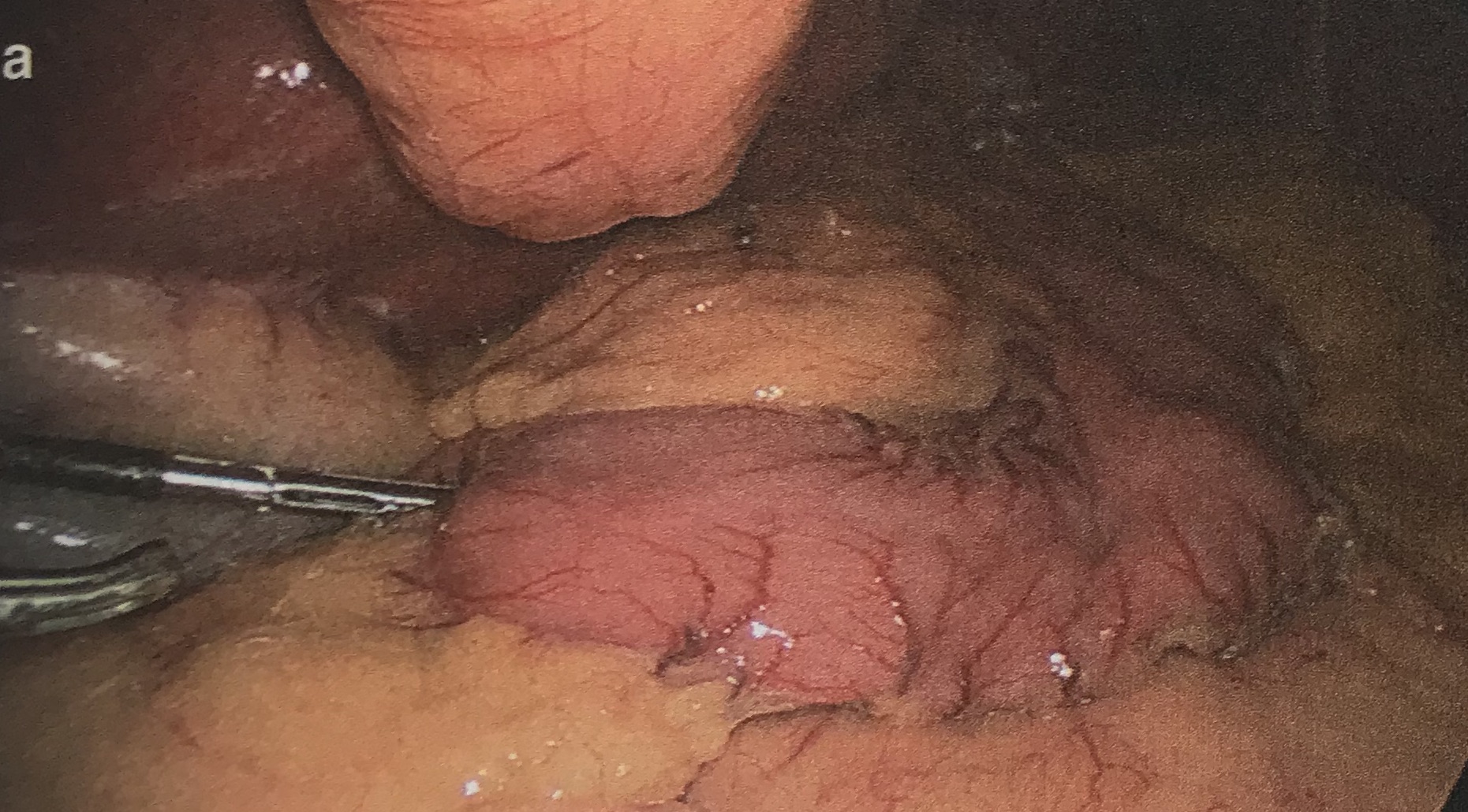
c. Create window to lesser sac at a point mid-way along the greater curve using 5mm bipolar/ultrasonic vessel sealing device
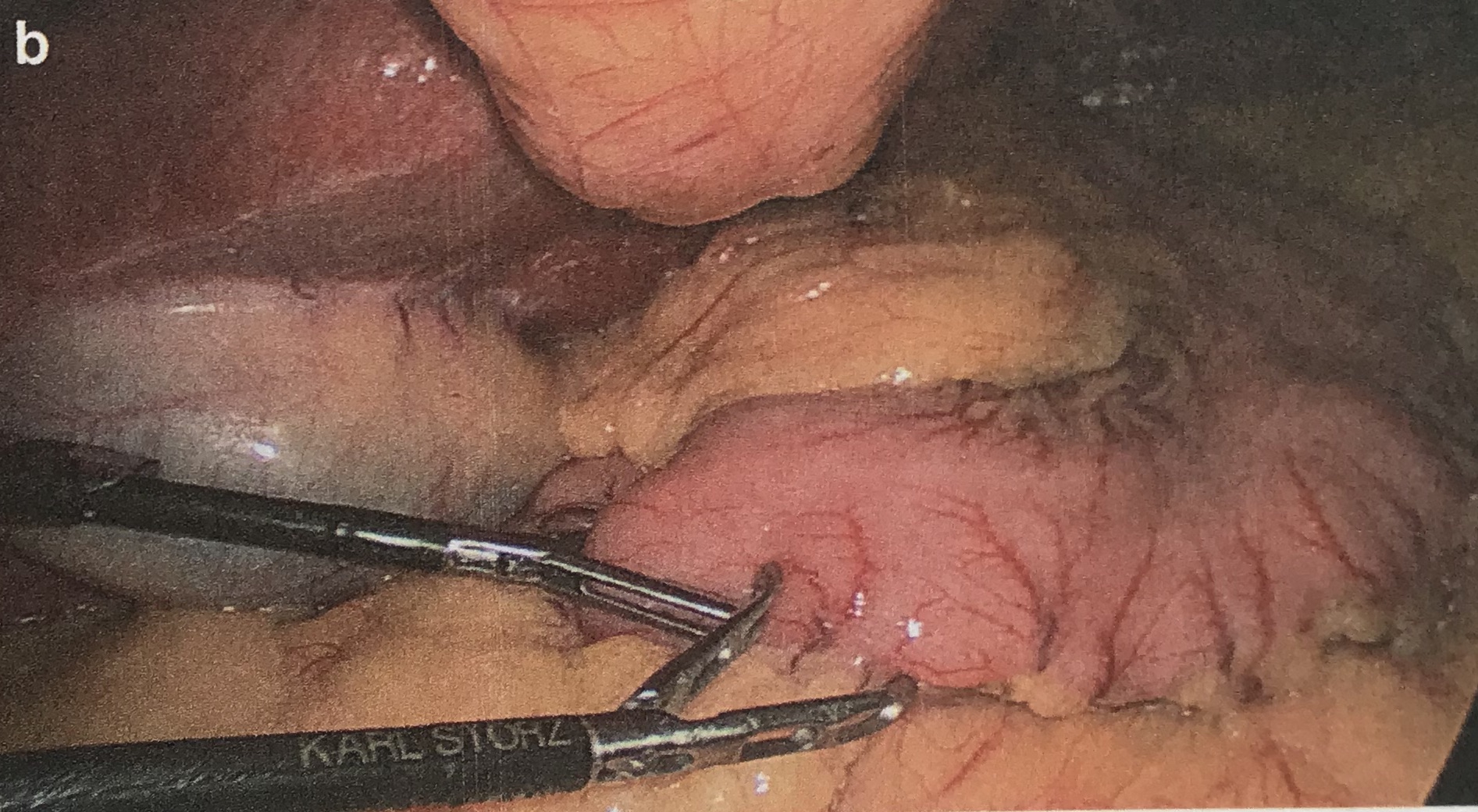
d. Continue to detach the greater omentum proximally, staying close to the gastric wall
e. Proceed to take down the short gastric vessels with care
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
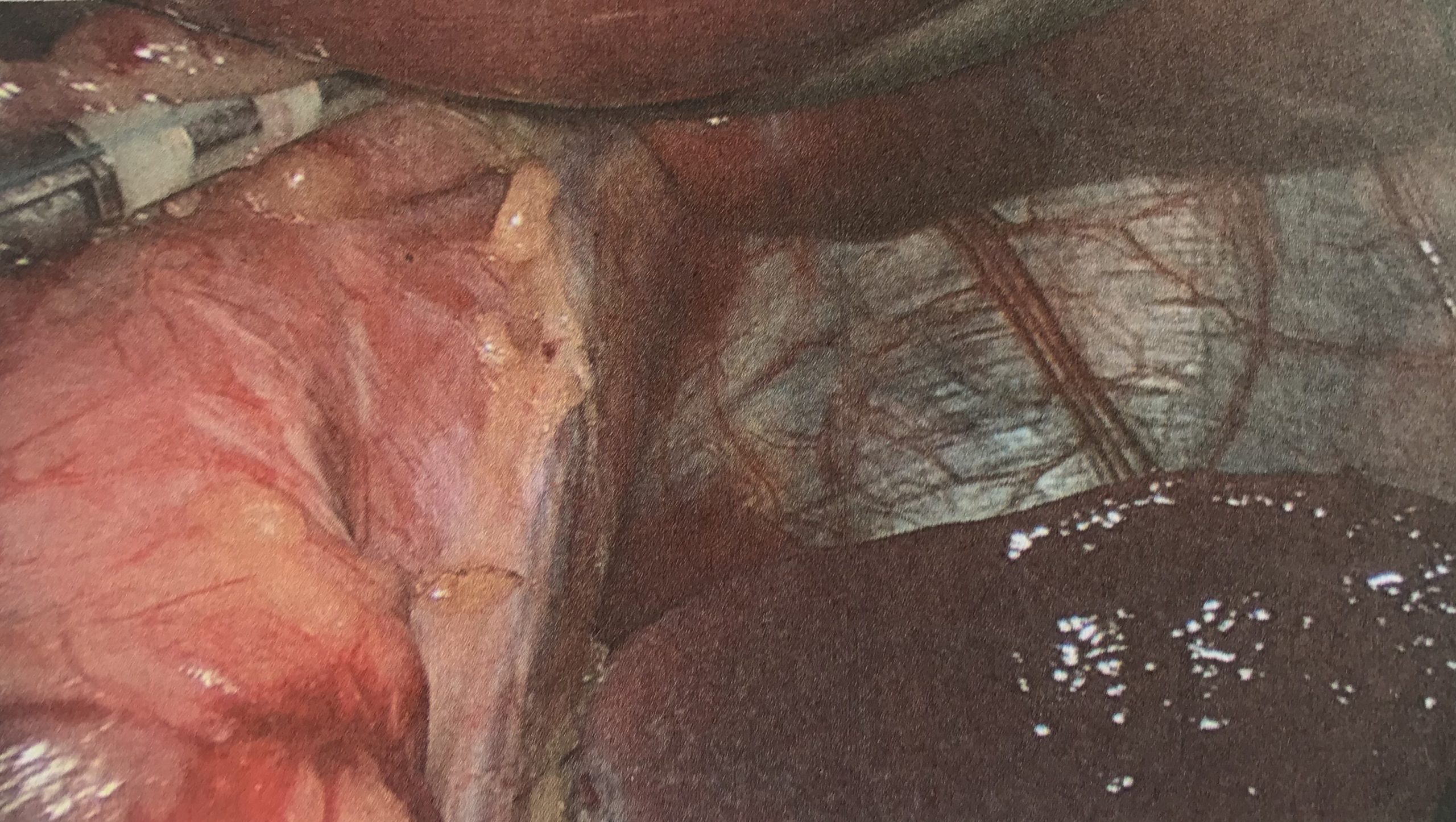
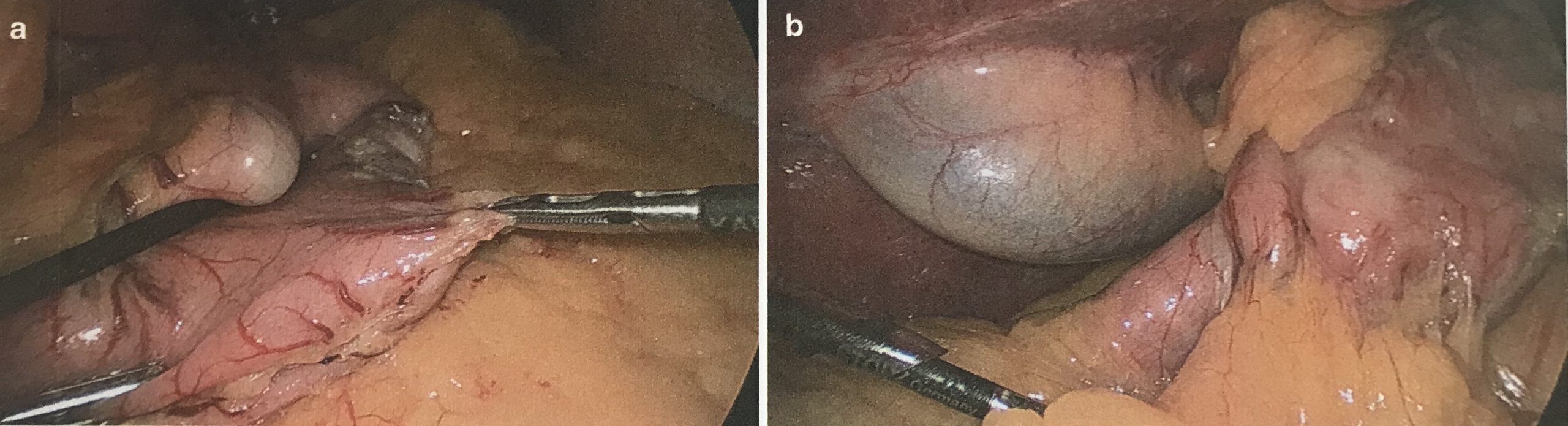
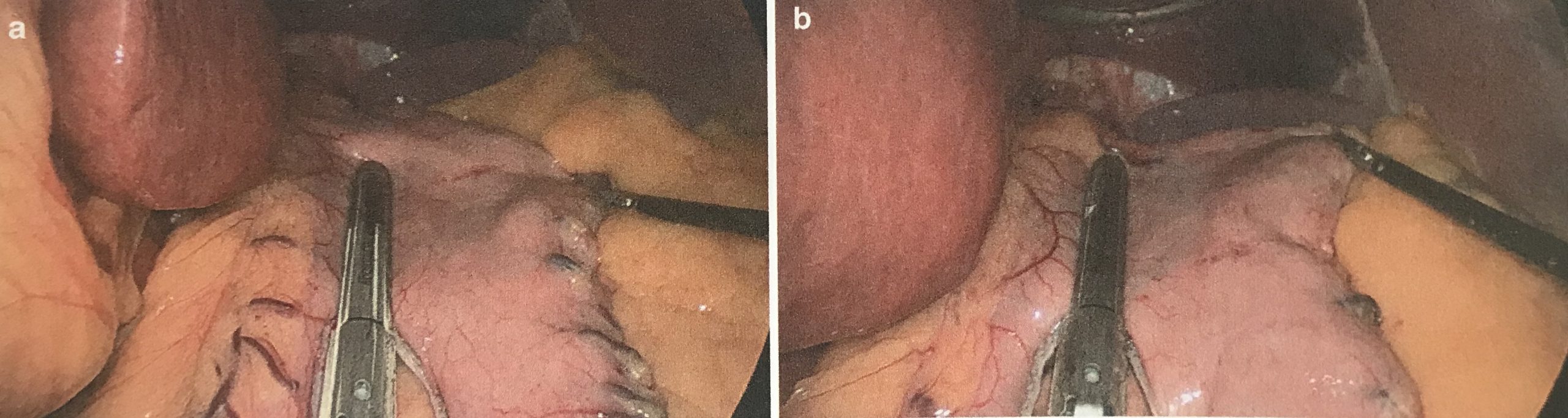
3. Dissection of Angle of His
a. Detach all adhesions to mobilise the fundus completely,
b. Expose the left crus completely to its medial border
c. Left-phreno oesophageal membrane defines the cranio-medial limit of dissection
d. Anteriorly, mobilise the oesophageal fat pad
e. Remove posterior attachments to the stomach and take care not to damage the left gastric artery (main vascular supply for remnant sleeve)
f. Then remove the distal portion of the greater omentum from the stomach – becomes thicker and vascular as it nears the pylorus. 2 distinct layers of omentum are encountered near this area, take them down individually.
g. Stop the dissection 3-5cm proximal to the pylorus (distance is variable)
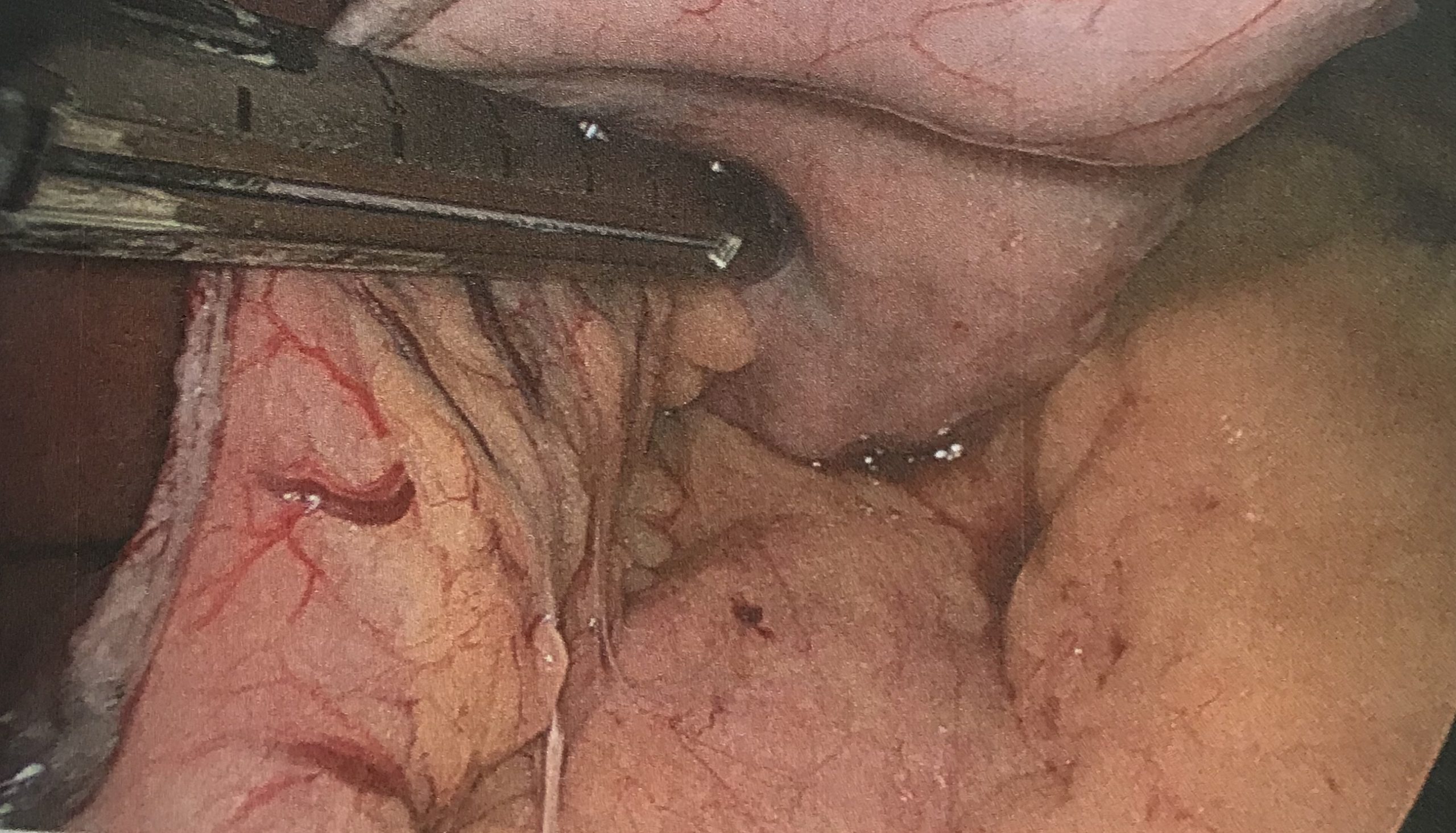
4. Creation of sleeve
a. Ensure all tubes placed in the stomach, except for the bougie are taken out (eg orogastric tube, temperature probe)
b. Advance the bougie to the duodenum under vision and ensure that it is straight (can be tricky, use atraumatic graspers to guide it and push through the pylorus)
c. Size of the gastric calibration tube ranges from 32 to 60 Fr. The smaller the tube, the higher the weight loss but also the leak rate and strictures.
d. For the first fire, place Endo GIATM stapler (purple cartridge) 3-5cm away from pylorus. Use this cartridge for first 2 firings (or black if stomach is thick).
i. Insert stapler through right-hand 12mm port
ii. Use left-hand to retract greater curve laterally (with assistant helping)
iii. Aim the stapler away from the incisura
iv. Before firing the first staple, distance from incisura is reassessed and ensure it is slightly away from the bougie at narrowing at this point can lead to a leak.
v. Wait for 30s before firing the stapler
e. The sleeve is created by sequential firings of Endo GIATM stapler using purple cartridges.
i. After each placement, rotate the stapler to check that excessive posterior stomach is not left behind.
ii. After each firing, check the line to make sure the formation is correct and there are no loose staples (which should be removed)
f. While retracting the stomach, the assistant should hold the greater curvature and not the anterior/posterior wall to ensure it does not cause twisting of the sleeve.
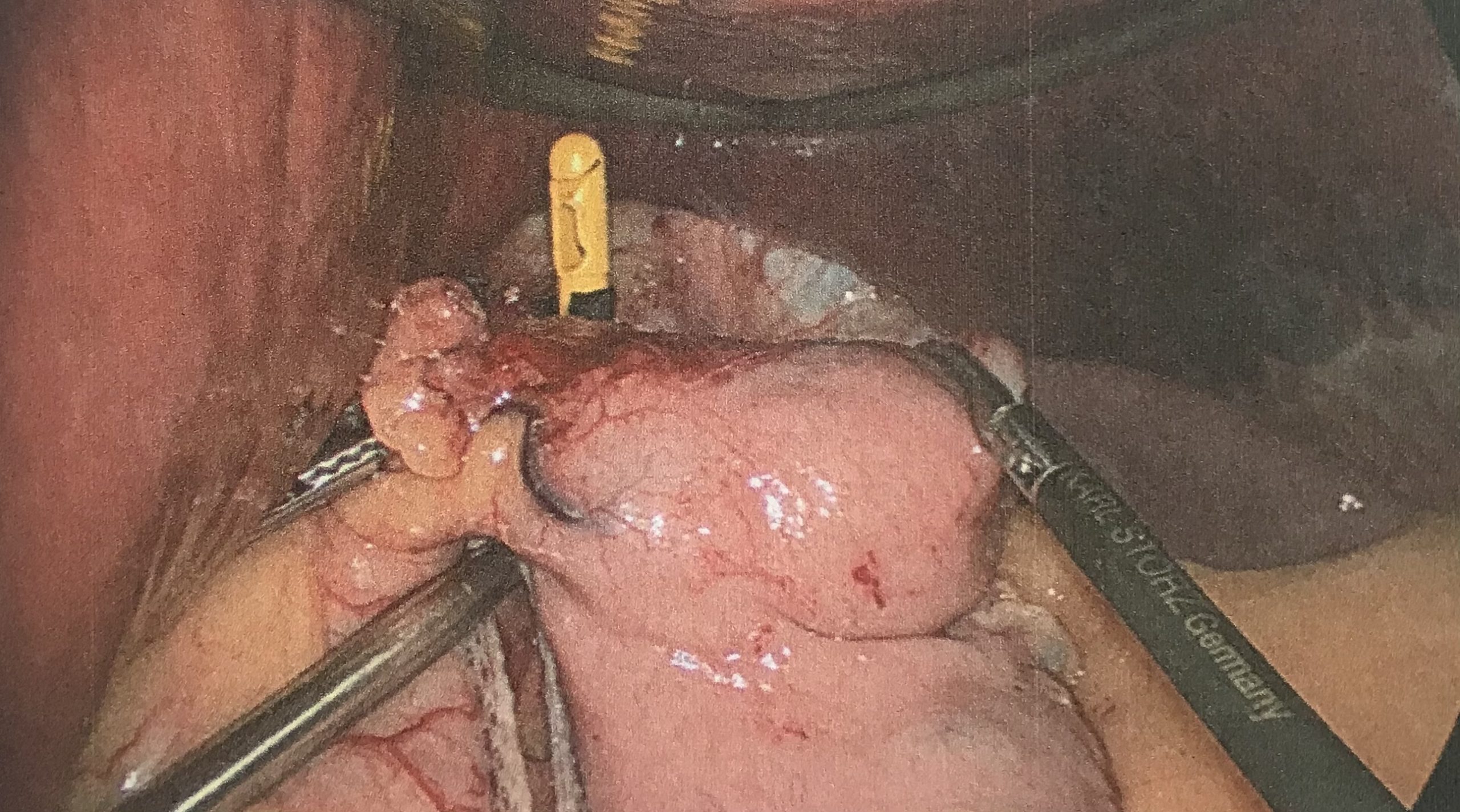
g. The last fire should be properly planned
i. An articulating instrument like Goldfinger is used to define the angle of His.
ii. Retract fundus to avoid bunching of tissues
iii. Take to include the whole of the fundus is resected as remnany fundus leads to poor longterm outcomes.
iv. Angle the stpaler away from the angle of His to avoid narrowing at the GOJ.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Haemostasis and reinforcement
a. Withdraw the bougie upto the GOJ before checking for haemostasis
b. Bleeders are controlled with small clips or figure of eight sutures to invert the bleeding age
c. Methods of reinforcement of staple line include oversewing, placing omental flaps and fibrin glue.
d. Buttressing materials are also available (Systematic review – absorbable polymer membrane is most effective at reducing leaks)
i. Gore Seamguard (glycolide trimethylene carbonate copolymer)
ii. Bovine pericardium strips (Synovis surgical Innovations)
iii. Porcine small intestine submucosa (Surgisis Biodesign)
iv. Worth considering in super obese, anticoagulants and OSA patients
2. Leak test and organ retrieval
a. Leak test can be done by air insufflation or instilling methylene blue dye (through bougie)
b. Specimen is retrieved through the right 12mm port after dilating it (+/- in a bag)
c. A Jackson Pratt 14Fr flat drain is place near the sleeve through left port
d. Right 12mm port closed using trans-fascial sutures and endo-catch
Post-operative care
– Monitor overnight in HDU
– Early ambulation (4-6 hours post op)
– SC heparin for DVT prophylaxis
– Deep breathing excercise to prevent atelectasis
– Sip clear liquids after 24h
– Discharged on 2nd/3rd day if tolerating liquid diet.
Follow-up:
– 1st review 1 week post-op
– Then, 1 month, 3 months and quarterly thereafter
– 6-monthly for 2 years
– Annual thereafter
– Nutritional monitoring is important with emphasis on dietary compliance and physical activity
– Support group meetings also effective
Note on complications
Haemorrhage
– can be extra-luminal from staple line, omental vessel, spleen injury, liver laceration or trochar sites
– Intra-luminal bleeding is uncommon and can be from staple line.
– Tachycardia, sudden hypotension, sanguinous drain output and drop in haematocrit are all suggestive
– Resuscitate and monitor obs and Hb/haematocrit serially
– If there is hypotension within 12hours of surgery, an urgent laparoscopy should be done
– Most can be managed conservatively if haemodynamically stable
Leak
– Classified as early or late, with cutoff of 3 days post-op
– Symptoms can be very variable
– Tachycardia, agitation, tachypnoea and fever are all suggestive
– Warrants contrast enhanced CT or gastrograffin study
– If diagnosed within 48-72 hours,
o re-laparoscopy
o repair the leak
o peritoneal lavage
o drain
o feeding jejunostomy is performed
– After 72 hours, repair is not recommended
o If stable, conservative management with image guided drainage of collections, parenteral antibiotics, NJ feeding, insertion of stents (silicon vs covered)
o If signs of sepsis, re-laparoscopy is necessary
– Chronic fistula will eventually require a surgical intervention, usually with roux-en-y fistula-jejunostomy, performed 3 months after initial operation.
Stricture
– Incidence 1-2%
– Can be acute or chronic presentation
– Most commonly at incisura
– In the early setting, might be due to oedema which settles (oversewing can lead to early vomiting)
– Chronic strictures may need multiple endoscopic dilatations
– If dilatations don’t work, conversion to a LRYGB is necessary.
Reflux
– Relationship between LSG and reflux isn’t clear
– Objective symptom scores and endoscopic findings seem to improve after LSG
– Hiatal hernia repairs should be done promptly.
Nutritional deficiencies
– Most commonly thiamine, Vitamin B12, Vitamin D3, zinc and folic acid.