Gastric Band Erosion
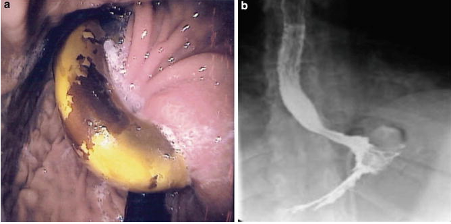
Always consider in port-stie infections.. especially late ones (>4 months)! It’s a very common finding.
Band gradually erodes through stomach wall into lumen. The cause might be injury to the stomach wall during placement or too tight placement leading to ischaemia.
You don’t get free air because the pseudo-capsule on the outside seals the perforation.
Most patients are asymptomatic, but can cause loss of restriction, nonspecific epigastric pain and GI bleeding.
Gastroscopy is the gold standard test.
Management:
1. Laparoscopic removal : divide adhesions, use tubing to get to band, cut and remove. This will leave a hole. You can use an omental patch for closure?
2. Transgastric approach: use a separate gastrostomy on the greater curve, find the band near the fundus, divide it and remove it. The gastrostomy can then be closed with a linear stapler. The smaller hole where some of the band and tubing would have been showing at the top can be left alone. The key here is that the encapsulation of the band has stopped sepsis and therefore you do not disrupt this area.
An alternative is to create a small gastrostomy for a laparoscopic balloon port to enter the stomach. With an endoscope to visualise and scissors through the port, the band can be cut on the inside of the stomach. Snare can then be used to retrieve the port, or it can be removed through the lap port (ideally 15mm)
3. Endoscopic removal – using an ERCP tools, you can pass a JAG wire around the band, then a stone crusher which can break through the band and split it! This can then be retrieved with an endoscope. The wire has to be divided through a skin incision for the access port.
The decision between 1 and 2 might depend on extent of band into the stomach and whether the buckle is on the outside (which might make transgastric removal more difficult).
Mr Nguyen:
1. Insert laparoscopic ports (he stands on patient’s left)
2. Remove the access port from outside and divide the tube
3. Use the band to find the gastric band.. which should be mostly just the tube coming out.
4. Insert endoscope – best viewed on retrofexion (in this case band was 80% inside the stomach)
5. Creates a hole with harmonic on anterior wall (make sure this is normal healthy stomach)
6. Suction out fluid, find the band and cut with scissors (+ diatherymy for some reason)
7. Use a toothed grasper to grab and remove. If the buckle is in the wall, will need some twisting motions to remove it.
8. Examine the entrance of the tubing.. it should look tiny and unremarkable, will heal up on its own.
9. Close gastrostomy with laparoscopic sutures, 2 layers, vicryl.
10. Repeat endoscopy and examine for leak
11. Retrieve the removed band through a 12mm port.
Video: https://watch.giblib.com/video/7439
(Shawshank12)