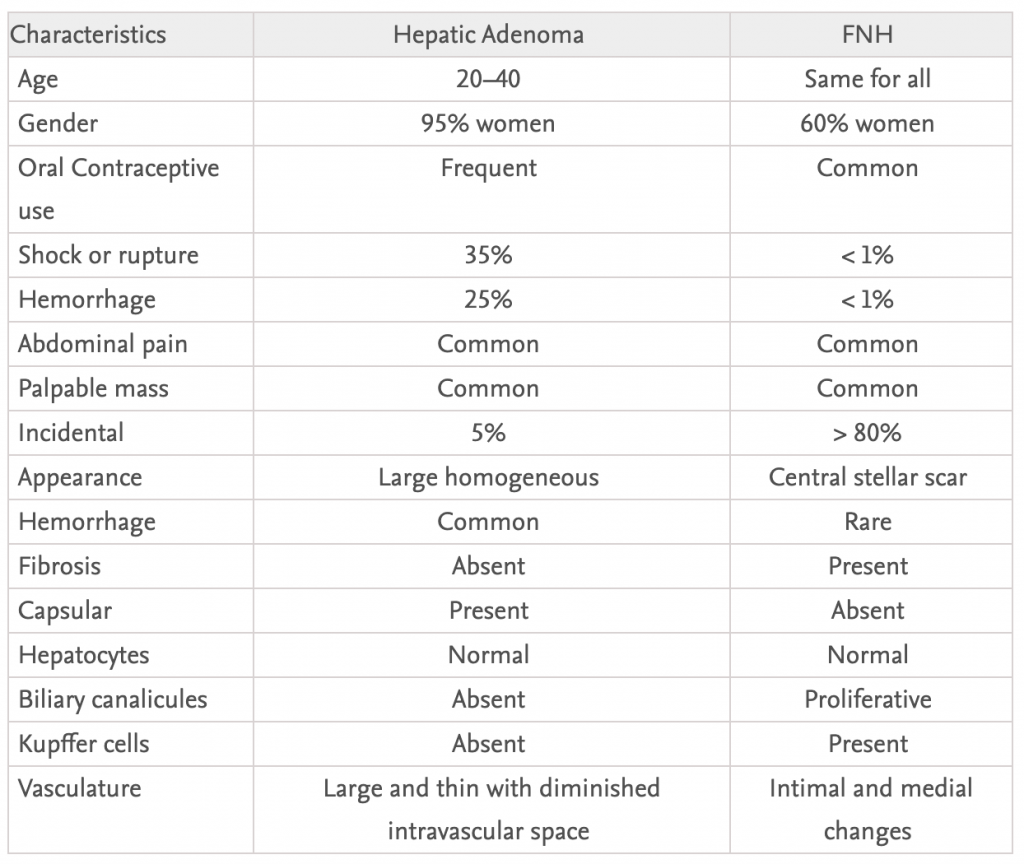
– primarily affects young women of childbearing age (20-40 years)
– often have a long history of using oral contraceptives (can regress after discontinuing but not consistently)
– also associated with anabolic steroid use, insulin-dependent diabetes and type 1a glycogen storage disease
– most commopn complication is intratumoral or intraperitoneal haemorrhage (occurs in 50-60% of patients)
– can undergo malignant transformation, can be detected by AFP
– elective resection has mortality of <1% but with rupture its 5-10%
– range in size from 1-30cm, average 8-10cm; the tumours are usually subcapsular, have superficial projections, occasionally pedunculated and are never nodular or fibrotic.
– normally hypervascular on CT and MRE but some can by hypovascular.
– contain vacuoles and glycogen but no Kupfer cells or bile ducts
– usually symptomatic causing pressure or haemorrhage
– can progress to adenomatosis which is inoperable or undergo malignant transformation
– only fine needle aspiration is advised for biopsy due to risk of haemorrhage
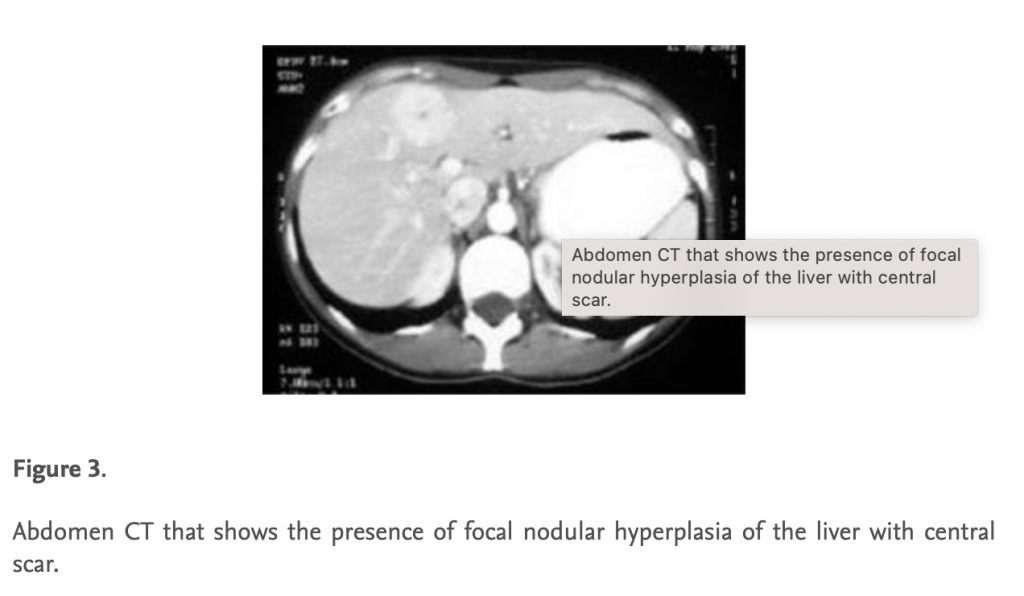
Focal Nodular Hyperplasia
– wider age distribution
– NOT associated with oral contraceptives
– Normally asymptomatic and rarely experience complications
– may be a precursor for fibrolamellar hepatopcellular carcinoma
– FNH is marked by a stellate scar, sometimes accompanied by haemagioma but is asymptomatic
– FNH takes up radionuclide, stains intensely on angiography and is safe to biopsy percutaneously.