Workup of pancreatic cystic lesions - IPMNs
Work up for cystic lesions of the pancreas – IPMNs
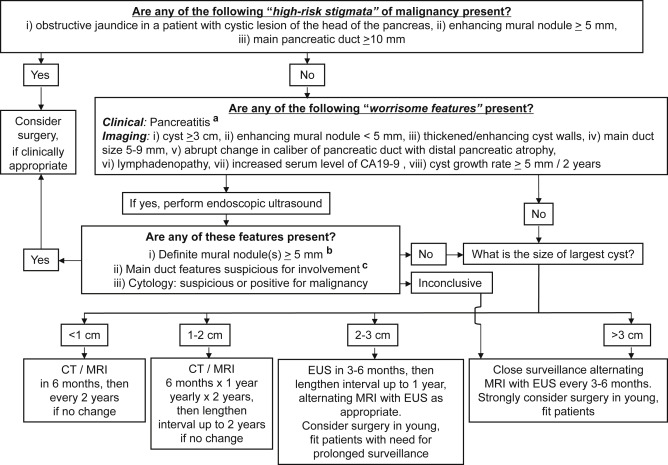
Fukuoka Guidelines 2017
– BD-IPMN are generally do not undergo surgery
– Some will become malignant
– Patients with IPMN are at higher risk for pancreatic ductal adenocarcinoma
– Hence, surveillance is carried out.
– If no significant change is observed after 5 years, stop surveillance
MD-IPMN are characterised by segmental or diffuse dilatation of the main pancreatic duct of >5mm without other causes of obstruction. (5-9mm “worrisome”, >10mm “high risk stigmata”)
Pancreatic cysts >5mm that communicate with the MPD should be considered BD-IPMN and should be differentiated from a pseudocyst in patients with prior history of pancreatitis.
If <5mm and asymptomatic, no further tests required but can be followed up.
If >5mm, a pancreatic protocol CT or Gadolinium-enhanced MRI with MRCP is performed. (MRCP is the best choice)
Symptomatic cysts have a higher risk of invasive cancer and HGD and therefore these require either resection or further evaluation.
“Worrisome features”
– Cysts > 3cm in size
– Enhancing mural nodule <5mm
– Thickened enhanced cyst walls
– MPD size of 5-9 mm
– Abrupt change in MPD calibre with distal pancreatic atrophy
– Lymphadenopathy
– Elevated serum CA 19-9
– Rapid growth of cyst >5mm/2 years
For these patients an EUS should be used for further evaluation – doppler EUS can demonstrate blood supply in mural nodule
“High-risk stigmata” on CT, MRI or EUS
– Obstructive jaundice in a patient with cystic lesion of the pancreatic head
– Enhanced mural nodule > 5mm
– MPD size of > 10mm
These should undergo further resection if surgically fit without futher testing.
All patients with cysts of £ 3cm without worrisome features should undergo surveillance according to size stratification (see flowchart below)
On EUS, suspected nodules may actually be mucin which would move with change in position and can be dislodged on cyst lavage. It would also not have doppler flow.
The presence of thickened walls, intraductal mucin or mural nodules suggests main duct involvement.
Use of EUS-FNA to obtain cyst fluid:
Elevated CEA distinguishes mucinous from non-mucinous cysts (but NOT benign from malignant)
Amylase is not elevated in IPMN
Serous cysts typically have low levels of CEA and amylase
Cytology can be diagnostic but sensitivity is low.
“high grade epithelial atypia” are suggestive (but not diagnostic) or a malignancy.
NB. In Japan, they would not FNA cysts with “high-risk stigmata” or “worrisome features” for fear of seeding.
When to resect?
Resection in BD-IPMN
– Mostly occur in elderly patients
– Rate of invasive cancer/HGD in resected BD-IPMN is 31.1%
– Annual rate of progression is 1-6%
– Therefore surveillance is reasonable
– Absolute indications are cytology positive for HGD and presence of mural nodules (5mm or more)
– Younger patients (<65) with cyst of >2cm may be candidates give cumulative risk of progression.
Indications for resection of MD-IPMN
– Frequency of invasive cancer/HGD in MD-IPMN is 61.6%
– Surgical resection is strongly recommended for all surgically fit patients with MPD >10mm, jaundice or mural nodules.
– Important to differentiate from chronic pancreatitis as it can cause dilated MPD.