Follow-up post bariatric surgery
8. Follow up
8.1 All patients will be contacted by phone within the first week of discharge by the bariatric practitioner. This point of contact is to establish whether there are any problems with recovery and to prevent unnecessary readmission to hospital. The phone consultation will follow a standard format and will cover all aspects of the immediate recovery. If concerns are raised the practitioner can discuss this with the consultant surgeon and has the option to bring the patient to clinic for a review, or book an early clinic appointment.
8.2 All patients will be followed up for a maximum of two years after surgery. Appointments will be made every 3-6 months within the first year with an option to alter the frequency depending on the patient’s progression. Blood tests will be performed at these appointments in accordance with National guidelines (see below). These results will be checked by the dietician or practitioner and the GP informed if there are any concerns raised.
8.3 Patients with gastric band will be seen at 6 weeks post-surgery for the first band assessment by the bariatric practitioner. Should there be concerns with the band or port position, then a band fill under fluoroscopic control will be made.
8.4 All patients with a gastric band will be offered a contrast swallow at 22 months post-operatively to ensure that the band is correctly positioned and adjusted to give adequate restriction prior to discharge back to primary care.
8.5 At the end of the 2-year follow up a discharge letter will be sent to the GP. This will formally summarise the patient’s progress from referral to discharge. It will outline the change in weight and BMI, improvement in comorbidities as well as formally handing over the care back to primary care. Information on long term follow up will be given including the need for lifelong vitamin and mineral supplementation and annual blood monitoring. Ways to refer back into the service will be outlined, but this will require separate funding to be established by the GP.
8.6 Should the patient need more intensive follow up, or the GP think that further input is required from the bariatric team the patient can be re-referred.
8.7 Any patient who becomes pregnant following bariatric surgery will be discussed in the next available MDT as per pregnancy pathway (see below). They will be offered an appointment with the dietician and close liaison will be kept between members of the bariatric and obstetric teams.
8.8 Should a patient with a gastric band need future non-bariatric surgery under general anaesthetic then their band will be managed depending on the type of operation and symptoms experienced. The bariatric practitioner can be used as a first port of contact for members of other surgical and anaesthetic teams for this.
8.9 Occasionally patients require revisional surgery converting one procedure to another (usually band to bypass). This is typically a two stage process of removing the band and completing the revision at a later date. Patients are offered an appointment with the practitioner six weeks following band removal when an assessment will be made of their suitability to proceed to revisional surgery and the pathway that they need to undertake for this.
8.10 The pathway and timings of revisional surgery will be made on a case-by-case basis. Individualised care will mean that patients will require differing lengths of assessment based on their medical, psychological and dietetic needs as well as clinical urgency and logistics of surgery. Patients will be required though to have a stable weight throughout this time period.
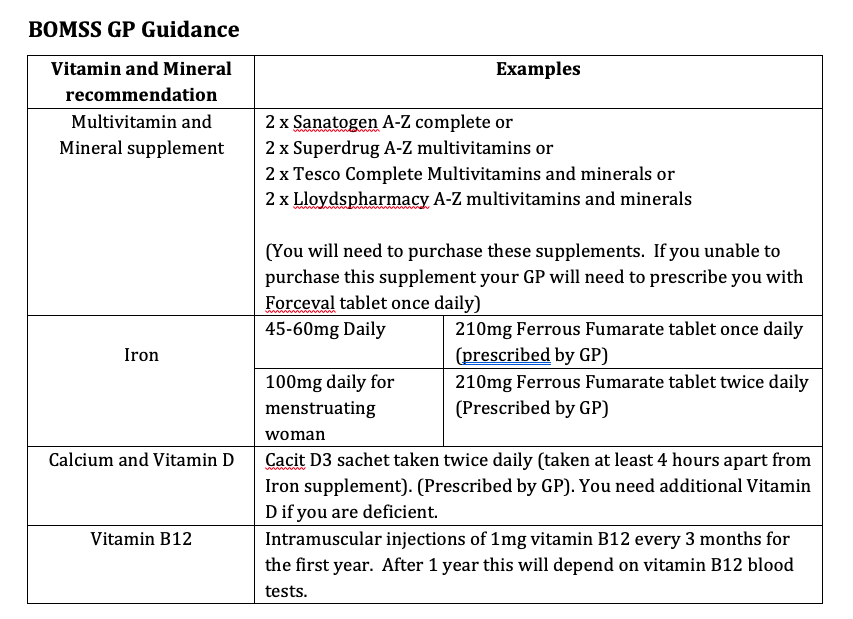
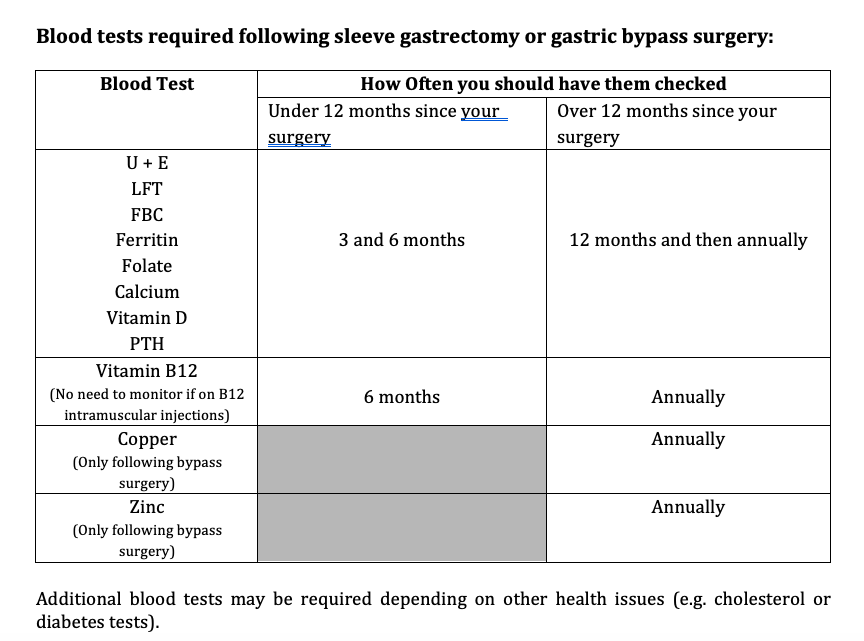
National Guidelines for supplements and blood tests post bariatric surgery