Nissen Fundoplication
Nissen’s – technique
Positioning and Ports:
Steep reverse Trendelenburg
Verress needle insufflation
Camera port is 10-12 cm (one hand breadth) beneath xiphisternum;
Operative ports: 5mm left sub-costal and 5mm right sub-costal; both in anterior axillary line
Assistant port: 5mm left mid-axillary line
Liver retractor: epigastric
1. Divide the pars flacida (Ligasure/harmonic)
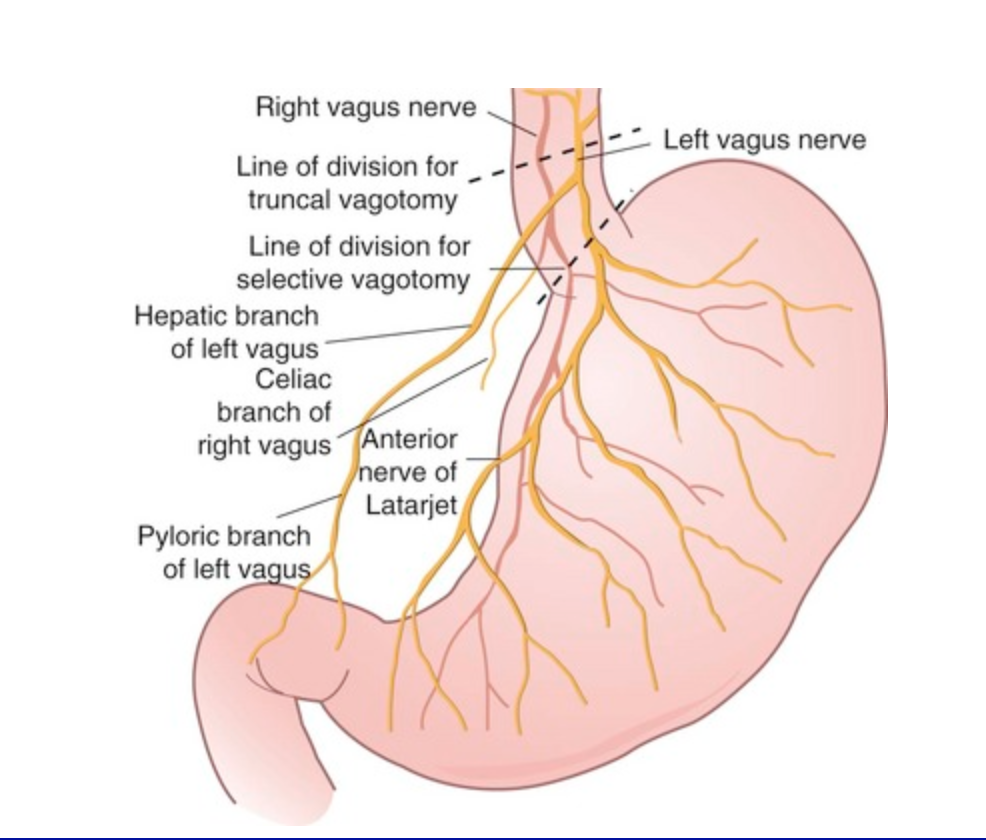
Pars flacida is divided and division of gastrohepatic ligament is continued superiorly, take care to not divide the vagal branches and any aberrant left hepatic artery.
Dallegmane says that in their series, by not dividing the hepatic branch of the vagus (which supplies the pylorus and the gallbaldder), they have found significantly lower incidence of bloating.
Look for the right crus through the window you have created and enter the plane between oesophagus and crus muscle.
2. Dissect around the hiatus
Expose gastrophrenic ligament by pulling down on GOJ fat pad. Divide phrenogastric ligament. Be careful when dissecting off the left crus, as the left/anterior vagus is very close to the left crus.
Incise the phreno-oesophageal membrane and make a retro-oesophageal window, dissecting between the aorta and the oesophagus. Take care to lift up the right (posterior) vagus nerve with the oesophagus and off the aorta. A penrose drain or nylon tape can be placed to provide caudal traction, as a sling.
3. Mobilise the oesophagus to get 2cm of oesophagus in the abdomen without tension (mix of blunt and sharp dissection with ligasure, use a swab or pledget if required)
Mobilise the oesophagus, starting posteriorly in the mediastinum and taking care not to damage the aorta, vagus nerves or pleura, until a minimum of 2cm of oesophagus lies in the abdomen without traction. TO do this, oesophagus should be mobilised upto the level of the inferior pulmonary veins.
If more length needed, can transect the vagus trunks. If this still doesn’t give enough length, a stapled-wedge Collis gastroplasty many be needed.
3. Mobilise the fundus
Hold the stomach greater curve anteriorly whilst assistant provides lateral traction on the greater omentum. Divide short gastrics 1cm later to greater curve with ligasure/energy device and work proximally along greater fundus to divide the splenic adhesions and free the fundus from the left crus.
Watson (Australia) published a randomised study on dividing short gastrics vs not during Nissens..found higher “wind-related problems” by dividing. But amount of division was not standardised.
3. Perform Hiatal repair (2-0 Ethibond, 12cm lengths, use sliding knots)
Right and left crura are approximated using permanent sutures, 2 or 3 sutures.
Take the lower most bite first – take large bites of the crus but avoid puncturing the aorta and the vena cava!
When tightening the knots, bring the muscles together, appose but don’t strangulate.
Can reinforce with PTFE pieces
Don’t angulate the oesophagus by placing too many posterior sutures. Consider one anterior suture. Leave it in the natural position.
How tight around the oesophagus? There should be some space when the nylon tape is pulled, but when relxed the oesophagus should fill the whole hiatus.
5. Create the wrap
Pass the mobilised posterior fundus behind the oesophagus and bring to meet the anterior fundus. This means only the anterior stomach wall should be in contact with the oesophagus. Ensure the shoe shine can be performed with ease.
Place 2 or 3 sutures to create a short and floppy wrap. Take an anchoring suture to the oesophagus at the attachments of the phreno-oesophageal ligament as this has some strength to it.
6. Closure
Close the fascia at 10mm sites, close skin
Post-operative:
Clear liquids day of surgery.
Free fluids on POD 1.
If tolerating fluids, discharge with sloppy diet for 2 weeks and then build up.
Full regular diet at 4-6 weeks.