Hyponatraemia
Causes:
Hypovoaemic:
· Vomiting
· Addison’s disease
Euvolaemic (ie. SIADH)
· Major surgery
· Meningitis
· Subarachnoid
· Head injury
· Pneumonia
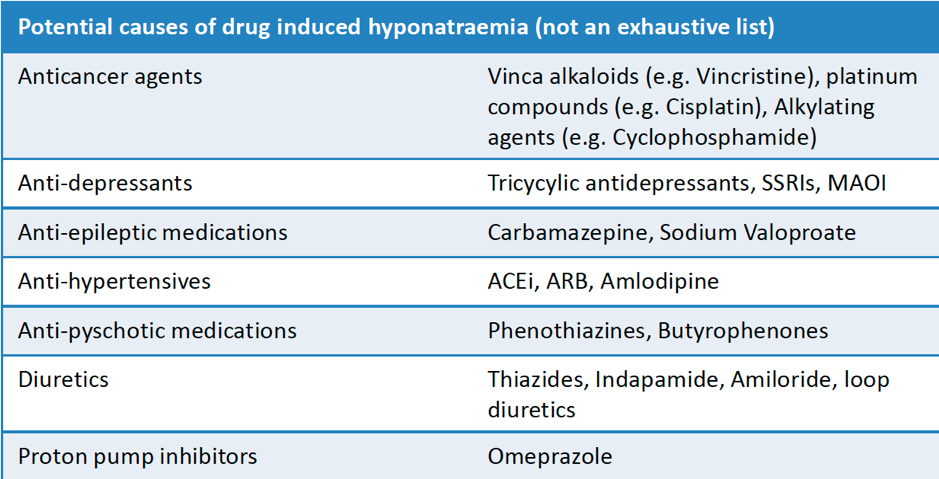
· Drugs
Hpervolaemiac
· CCF
· Cirrhosis
· Nephrotic syndrome
· Myxoedema
[Gloucester Hospital guidelines]
Na < 130mmol/L is significant
Symptoms usually occur when <125 mmol/L
General steps:
– Clinical assessment
– Bloods to include
o Renal function
o Serum osmolality
o Glucose
o Cortisol 9am
o TFTs
o LFTs
– Urine osmolality and urine Na
– Review drug charts and stop contributing meds
– Review fluid charts – stop use of dextrose infusions
Acute Hyponatreaemia:
Acute symptoms: CNS disturbance, confusion, headache, drowsiness, reduced GCS, seizures, encephalopathic
Treatment:
– Ideally move to a level 2 monitored bed
– If Na<120 mmol/L AND no other cause identified,
o Administer 1.8% hypertonic saline 150ml iv over 15 minutes
o Aim to improve symptoms rather than correct Na
o Repeat VBG after 20mins and if no change in Na, give further bolus
– Re-check Na at 6, 12, 24 and 48 hours
o Na should not rise > 6mmol/L in first 6 hours or > 10mmol/L in first 24 hours
o If rapid overcorrection, use IV dextrose or consider desmopressin
Chronic hyponatraemia
Assess hydration status: hypovolamic, euvolaemic or hypervolaemic
Hypovolamic:
o Treat with 0.9% saline
Hypervolaemic:
– Treat underlying cause eg. CCF, renal failure, liver failure
Normovolaemic:
– Check plasma and urine osmolalities
o Plasma <275 mOsm/kg AND Urine >100 mOsm/kg = Hypotonic Hyponatraemia
§ Check urine Na+
· Urine Na>20 = Likely SIADH
· Urine Na<20 = Re-consider hypo/hypervolaemia
o Plasma >275 mOsm/kg = Hypertonic hyponatraemia
§ Consider hyperglycaemia (eg.HHS), mannitol infusion
o Urine Osm < 100 = consider primary polydipsia
Safe limit of correction is 10mmol/L in first 24hours and then 8 mmol/L in subsequent days.
Groups more at risk of osmotic demyelination are elderly patients, children <16, malnourished, alcoholics, CNS disease and post operative patients. Have a lower rate of correction in this group.