Obesity surgery
Criteria:
BMI > 40
BMI 35-40 with co-morbidities
BMI any good?
Reproducible method but it doesn’t measure body fat percentage
In muscly adults, BMI will overestimate
It’s a poor predictor of cardiovascular risk
<20 Underweight
20-25 Idea
25-30 Overweight
>30 Obese
>40 Morbidly obese
>50 Super obese
Patient choice should determine type of operation. They should be fully informed of short and long-term outcomes and should attend patient groups to discuss operations with others who’ve undergone them
Impact on diabetes is seen most dramatically after biliary pancreatic diversion with duodenal switch (97%) and bypass (85%). According to the NBSR, 65% should be able to come off all diabetic medications.
The reason is probably likely multifactorial but the immediate resolution in the post-op period is likely to be due to re-routing of nutrients and the changes in hormones that it causes and because of changes in GLP-1
Weight loss following bariatric surgery:
BPD/DS mean excess weight loss of 70%
Bypass 62%
Banding 47.5%
Also, substantial reduction in mortality from the resolution of co-morbidities such as diabetes and hypertension, as shown by number of studies including Swedish Obese Subjects Study. Greatest reduction in mortality is fron reduction in cancer related death (60% reduction in 7 years)
Mortality:
0.1% banding
0.5% bypass
1.1% BPD/DS
Sleeve gastrectomy
- Quick and safe
- Can progress to a bypass later
Ghrelin: produced by the gastric fundus, reduced in sleeve resection and results in less hunger. However, in bypass studies haven’t shown a change in ghrelin
PYY and GLP-1 seem to control appetite as well.
LRYGB
Gastric pouch on lesser curve <30ml
Gastrojejunostomy – retrocoloic, stapler
Jejunojejunostomy
Mesocolic, Petersen’s and JJ mesenteric defects
Cholecystectomy?
3% get gallstones (accelerated by rapid weight loss)
Adhesions make it more difficult at a later date
Endoscopic access to biliary tree is more difficult
Complications of bariatric surgery
Gastric band:
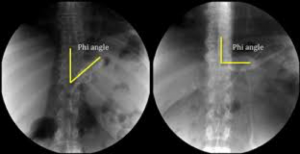
slippage – stomach prolapses through band and can get strangulated, looks more horizontal on x-ray. The phi angle should be between 45-58O, if it slips its larger.
Initial management: resuscitate and deflate the balloon to completeness (ideally with Huber needle..not necessarily in slips as band is likely to come out). If symptoms aren’t alleviated, it’ll need complete removal. (remove fibrous reaction around head of band, cut the buckle of the band behind the locking head/undo locking head and pull band through. Access port will also need to be removed)
Erosion: Obtain a plain x-ray/contrast swallow/OGD
Gastric bypass – need full assessment to determine the cause. May be internal hernia, adhesions, related to malnutrition and lack of vitamin supplementation.
CT scan with contrast
If no cause identified, a diagnostic laparoscopy
Peterson’s hernia – small bowel loops in the space between gastro-jej and the transverse colon (<3% incidence)
Other potential spaces are behind the biliopanceatic limb and roux-limb at the jej-jej anastomoses; if retrocolic anastomosis, defect in mesocolon.