High Resolution Manometry Interpretation (for surgeons)
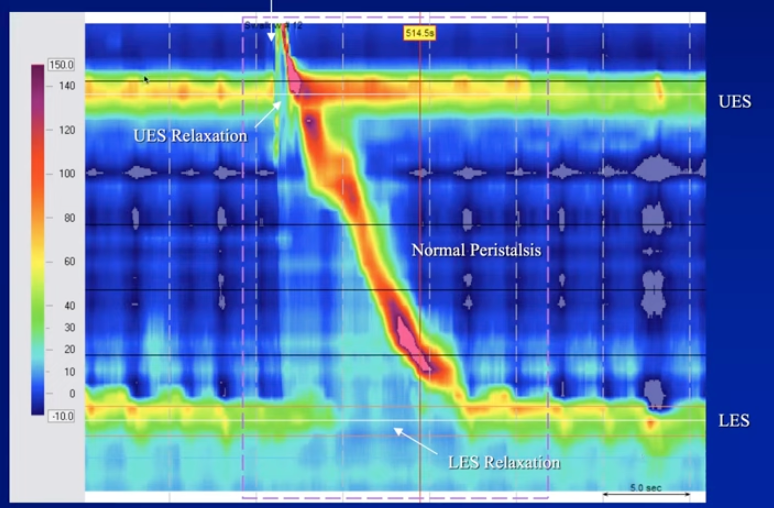
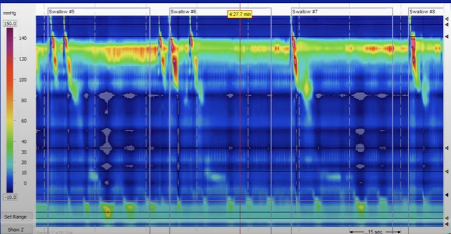
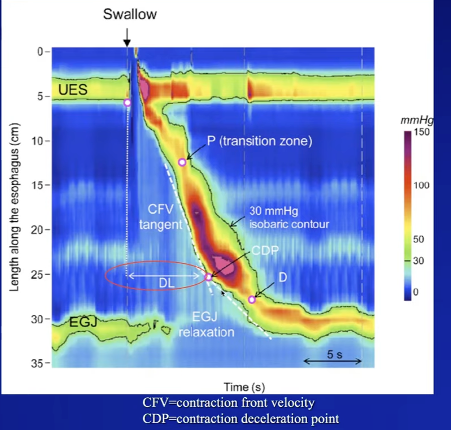
The Normal swallow:
y-axis – length along oesophagus,
x-axis – time in seconds
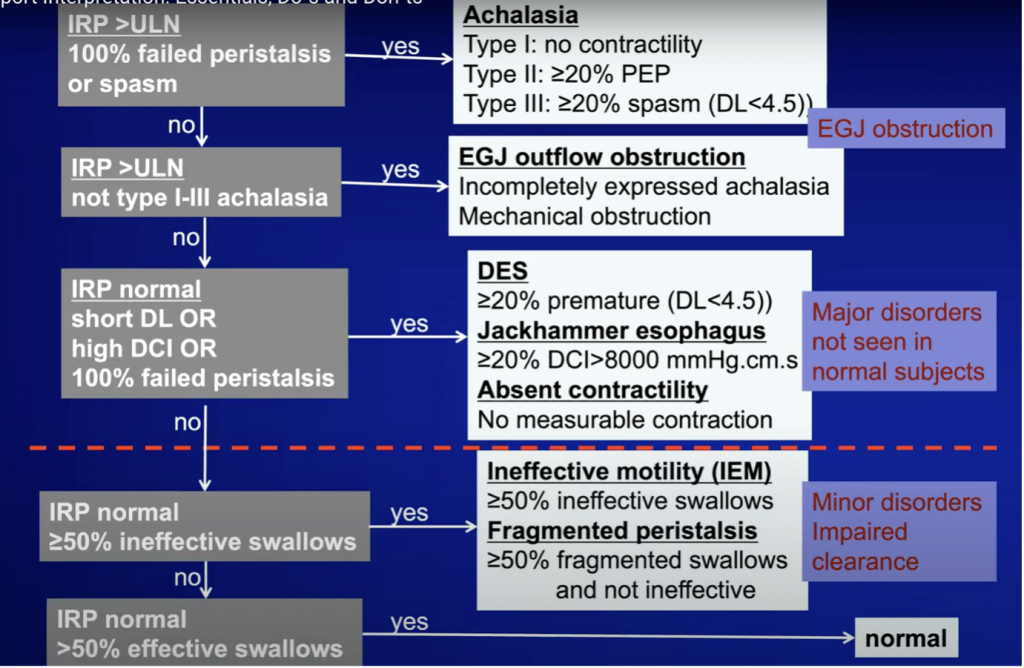
Chicago classification Version 3.0 (soon to have 4.0)
3 main metrics: IRP, DCI and Distal latency
1.IRP – integrated relaxation pressure; pressure at LES across the swallowing episode.
It takes 4 second intervals’ lowest pressure across several channels to give this value. It therefore minimises any influence exerted by the diaphragm or by the food bolus being present.
Normal IRP <15 mmHg (with Medtronic system)
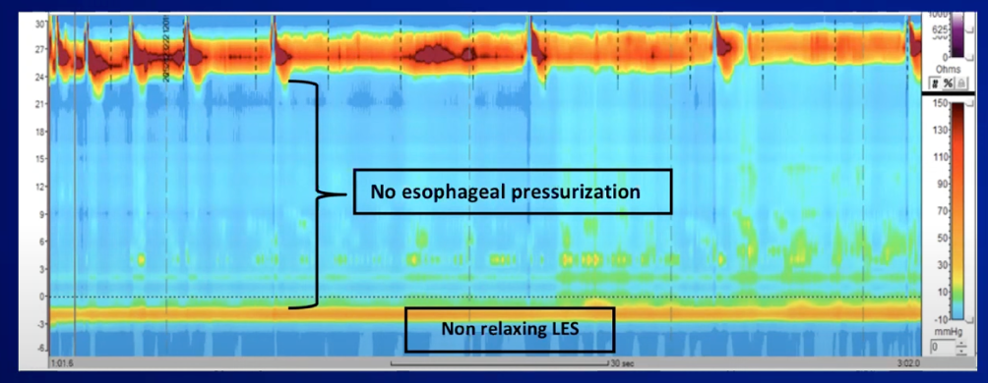
a. Abnormal IRP in Achalasia- Type 1
–Higher than upper limit of normal
–Absence of ANY normal peristalsis
–No relaxation of LES
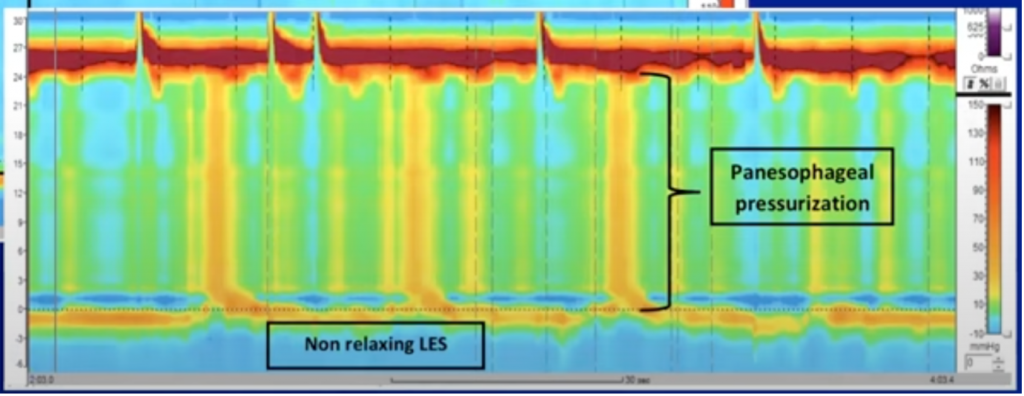
b. Type 2 Achalasia
–Panoesophageal pressurisation
–Non-relaxing LES
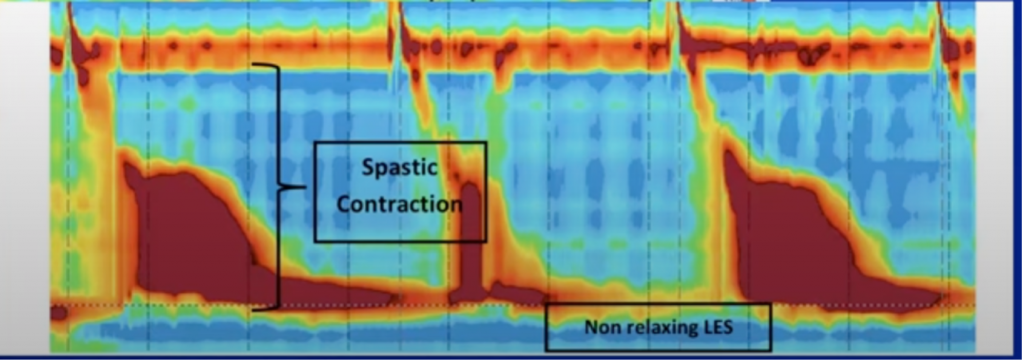
c. Type 3 achalasia
–Spastic contractions
–Non-relaxing LES
d. EGJ Outflow Obstruction
IRP is higher than normal but there is at least some normal peristalsis.
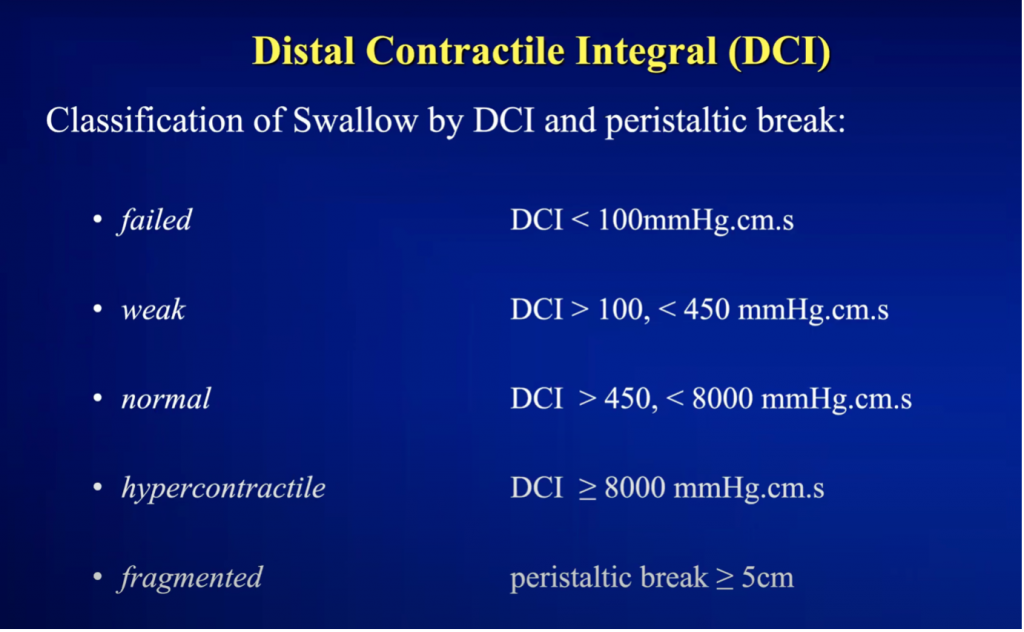
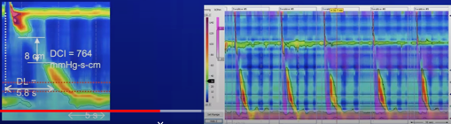
2.Distal Contractile Integral (DCI)
Measure of the overall strength of persistaltic contraction
Accounts for the length, amplitude and duration
a. Hypertensive peristalsis (“Jackhammer”) : at least 20% have DCI >8000 mmHg.cm.sec
NB. Nut-cracker is no longer recognised in Chicago
b. Absent peristalsis: all swallows have DCI <100
c. Ineffective oesophageal motility – at least 50% are weak or failed
d. Fragmented peristalsis – at least 50% of normal swallows with normal DCI have more than 5cm peristaltic break
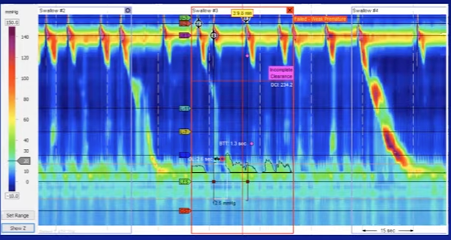
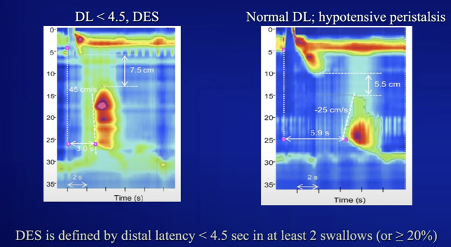
3. Distal Latency
Time between onset at UES relaxation and start of the distal peristaltic segment
Normal is 4.5 seconds or more
Hence <4.5 secs is premature contraction (“spasm”). This is important, because when diagnosing ‘distal oesophageal spasm’, at least 20% of swallows must have DL less than 4.5secs. As opposed to a hypotensive peristalsis where there is a peristaltic break but DL is normal.
The hierarchical approach
A.EGJ outflow: look first at the IRP.
a.Type 1 achalasia: absent peristalsis
b.Type II achalasia: ³ 20% panoesophageal pressurisation
c.Type III achalasia: ³ 20% premature sequences
d.EGJ outflow obstruction: intact body peristalsis
Obstruction: median IRP ³ upper limit of normal (ULN)
Caveats – achalasia needs to be considered if IRP < ULN in the setting of absent peristalsis
Tumours at GOJ can also cause EGJOO and if clinically indicated, need further investigations.
NB. In patients with paraoesophageal hiatus hernias, there will be EGJ obstruction, but this will be clinically insignificant