Repair of giant hiatus hernia

Tips:
1. Place all your ports higher than you normally would
2. Extra 5mm port 8-10cm below right subcostal – for assistants to pull down sac from both sides whilst surgeon has both hands free for dissection
3. Keep a pressure of 12mmHg as too high can cause cardiac compression, pneumomediastinum, cervicofacial surgical emphysema and hypercapnoea.
4. In type III hernias, its often not possible to get the >2cm abdominal oesophagus
5. manometry can suggest if there is oesophageal shortening (the distance between UES and LES averages 20.5cm in normal people)
6. Request anaesthetist to wake the patient gently to avoid retching
Procedural steps:
Preparation
1. Reverse Trendelenburg position
2. Attempt to insert NG tube for decompression, although this might not be possible under the stomach is reduced
Ports
Operative
1. Reduce the contents into the abdomen, the assistant will have to maintain the stomach in the abdomen once reduced (although the cardia, gastrosplenic ligament and some short gastric often stay in the chest)
2. Dissect the sac anteriorly and left laterally until the anterior and left side of oesophagus is identified .. remember to preserve the left pleura and the anterior vagus nerve, gradually free the sac off the left crus completely and approach posteriorly
3. Retract the patient’s lesser omentum to the patient’s left and start by dissecting the hernia sac off the right crus (standard approach through window in pars flacida) and gradually clear the hernia sac off the right pleura, right oesophagus and the posterior vagus nerve.
4. The sac can then be retracted laterally and upwards to dissect between the oesophagus and the aorta
5. Division of short gastric is usually not needed
6. Once the sac has been detached from the oesophagus and mediastinum, its either brought back into the abodmen or resected, depending on the size of the sac. A large lipoma is usually found around and must be removed to allow dissection of the lower oesophagus. the posterio vagus nerve has to be preserved with the oesophagus
7. Its usually necessary to dissect the lower oesophagus from mediastinal attachements as well as the sac to allow 1-2 cm to sit in the abdomen. (NB. if short oesophagus, the vagus nerves can be divided but along with pyloroplasty/pyloromyotomy)
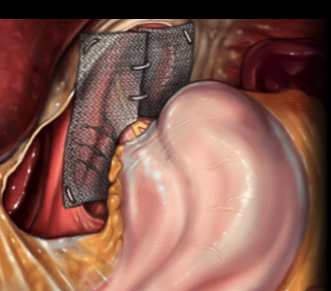
8. To prevent intrathoracic migration, the hiatus is closed with sutures +/- pledgets +/- mesh. If mesh is needed, use PTFE as it produces fewer adhesions. Close the hiatal defect posterio to anterior using interrupted non-absorbable sutures (0-Ethibond). Normally 3-5 sutures are required. IN huge hiatal defects, 1 to 3 suture are also applied anterior to the oesophagus. (NB. if a bougie is considered, 50Fr)
9. To reinforce the repair, a 15x10cm vicryl (or even polypropylene) mesh with a slit along the middle leading to a 3cm hole can be fashioned and refixed around the oesophagus with staples or non-absorbable sutures.
10. Funodplication is necessary as 30-40% have reflux and at least 20% will get reflux after the operation. You have to take care to perorm the wrap over teh oesophagus and not over the hernia sac
11. Gastropexy can be performed by fixing the fundoplication to the crura / the cardia or fundus to the diaphragm / fixing stomach to the anterior abbdominal wall (although this last one isnt show to reduce recurrence rate and can cause post-op complications).
– eg. fix fundoplication to cura with 2 or 3 non-absorbable sturues, but only if crura is good quality (nb. fundoplication can be fixed onto the mesh as well)
12. Drain the mediastinal space if there is oozing
Post-op
CXR if difficult op to rule out pneumothorax or assess severity of pneumomediastinum
Anaesthetic reversal should be smooth to avoid retching!
Leave NG tube in place for 24-48 hours to minimze risk of gastric dilatation? with soft diet starting once tube is out
Avoid physical exertion for 1 month
Typical postop stay for laparoscopic is 3 days (vs 9-10 days for open)
Indications:
Giant HHs have a high rate of symptomatic issues such as compression on mediastinal structures, GI bleeding, ulcer, stricture of perforation. Thus, most would agree that they should be repaired.
Consider repairing if
– compression of mediastinal organs (dysphagia, arrhythmia, chest pain)
– dysphagia
– GI haemorrhage (haematemesis, melena or anaemia)
– obstruction due to stricture or volvulus
– oesophagitis secondary to hernia
– asymptomatic – if young or medically fit
NB. Barrett’s is considered a relative contraindication for the laparoscopic approach.. why?