TAPP Inguinal Hernia Repair
Supine positioning with 20 degrees head-down tilt
Supraumbilical 10mm port
7cm lateral to this, insert 5mm at same level on ipsilateral side and 2-3 cm below this level on contralateral side
[if bilateral repair, insert both at same level]
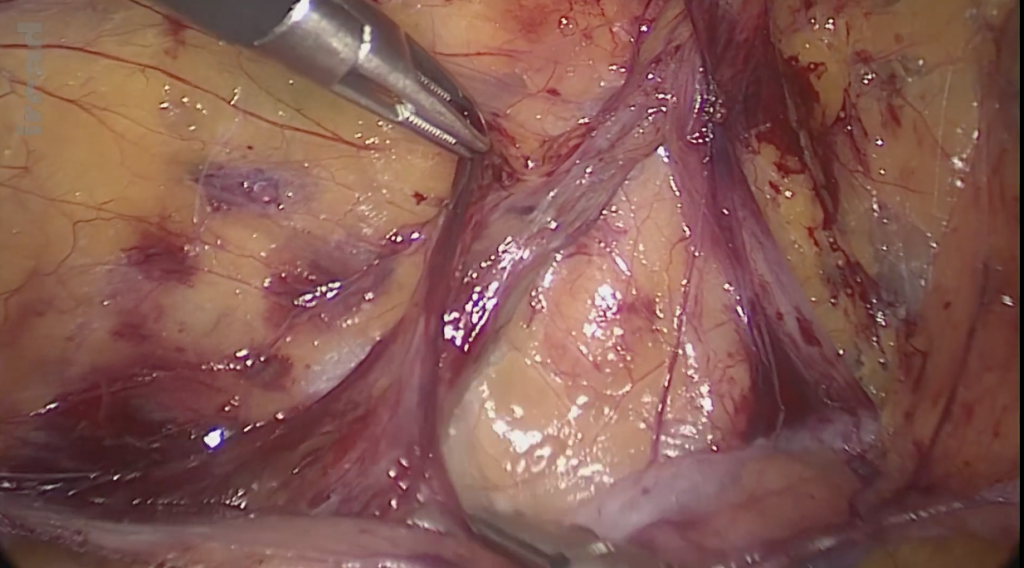
Identify anatomy and examine the indirect and direct hernia orifices
Mark line of division from ASIS to medial umbilical ligament using hook diathermy. (mark out with dots in fatty patients)
Open the peritoneum and allow gas to enter. Use the landmarks to divide peritoneum to the medial most extent and then make a vertical (upwards) split.
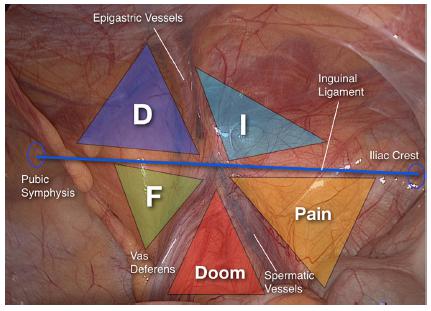
Take care not to divide the epigastric artery.
Using Maryland with diathermy, swipe away the fat from the peritoneum. Its very important that you do not enter a tunnel within the fat. Divide any adhesions with diathermy.
Keep checking intraperitoneally to ensure the peritoneum is being separated from the structures. The vas and vessels WILL BE peritonealised and therefore they have to be forced off the peritoneum.
Medially, to identify the pubic tubercle put your Yohannes in and lift upwards whilst sweeping the tissue down with the other hand. This avoids damage to the bladder.
YOU NEED 2-3 cm CLEARANCE BELOW THE PUBIC BONE. This is where the medial recurrences occur.
Lower the peritoneal flap to a horizontal line with the ASIS. Inferiorly, the vas deferens should meet with the umbilical artery.
For the hernia, everything internal of the transversalis fascia should be reduced, to avoid any lipoma remaining in the hernia.
HN notes: when reducing the peritoneum through the deep ring, there will be a ‘tent’ going into the tunnel, you should be able to sweep everything off it. Start anteriorly, then laterally and then finally on the medial side, towards the feet, until the instrument can get behind it and travel to the other side. One of the structures you sweep off it ON THE MEDIAL SIDE will be the Vas.
AVOID THE CORONA MORTIS.
IF there’s a large lipoma of cord, it should reduce with minimal diathermy. However, be careful when dissecting it off the cord as vessels including the artery can be running in it! Peel lipoma off the vessel!
Insert the mesh and insert absorbatek to just above the pubic bone to the ant abdo wall and further ones along the superior border. (AVOID THE IEA and superficial nerves running along the wall). You can also fix the transversalis fascia to the internal abdo wall.
Close the peritoneal flap with further tacks..stay superficial.
Deflation under direct vision.