Laparoscopic Roux-en-Y Gastric Bypass (Linear Technique)
Pre-procedure
Liver shrinkage diet
Informed consent
Thromboprophylaxis
Prophylactic antibiotics
On-table setup and positioning
Liver shrinkage diet commences 2-4 weeks prior to surgery. Low calorie and low carbohydrate. It reduces liver size and thereby improves access and reduces abdominal wall splinting.
Informed consent should include…
– Benefits of the operation
– Specific risks (bleeding, infection, port-site hernia, visceral injury, need for conversion to open, anastomotic or staple line leak, internal hernia, dumping syndrome, gastric or stomal ulceration, anastomotic stricture, malnutrition with the need for lifelong vitamin and elemental supplementation)
– General risks (GA, DVT/PE, atelectasis, pneumonia, MI, stroke, anaesthetic complications and mortality risk <1:300)
– Alternative procedures if bypass cannot be done (sleeve gastrectomy, abandon)
Thromboprophylaxis: use of stockings for 30 days postoperatively, LMWH preoperatively and then for 7-14 days postoperatively. Lower limb flow-trons intraoperatively and immediately post-op.
Prophylactic antibiotics: are routinely given at induction and continued for 2 postoperative doses
Positioning of patient: reverse Trendelendburg position with split approach. Operating surgeon stands on the right side of patient with assistant between the legs. Scrub nurse on left side. Laparoscopic monitor is positioned just above patient’s head in the midline. An orogastric (30Fr) is inserted to decompress the stomach (which will be drawn back before stapling)
Verris needle in left mid-clavicular line just below costal margin
Aim for insufflation upto 15 mmHg (12-20 mmHg)
– Avoid pressures more than 15 unless for short periods
Four 10/12 mm trocars and a liver retractor are placed
– First in the midline, 15cm below xiphisternum (optical, non-bladed)
– Second trocar in the left flank, one hand’s breadth to the left and slightly higher than midline port
– Third trocar in RUQ, midpoint between first port and costal margin
– Last trocar in LUQ infero-lateral to Verris needle site
– 5mm incision in epigastric for liver retractor
Diagnostic laparoscopy
– Hiatus hernia? If so, do a cruroplasty before starting bariatric op.
– Abdominal adhesions – is the small bowel mobile enough to reach the stomach?
Intraprocedural
Formation of gastric pouch
Creation of a gastrojejunal anastomosis
Creation of the jejuno-jejunal anastomosis
Other essential steps – closure of hernia defects and leak test
These steps can be done in a variety of orders
A key step is often dividing the omentum to prevent undue traction on the anastomosis (longitudinally upto the transverse colon)
Variations are
– anastomosis technique (linear vs circular vs hand-sewn),
– alimentary limb configuration (antecolic vs retrocolic, antegastric vs retrogastric),
– length of biliopancreatic and alimentary limbs
o BP limb 25 vs 50 vs 100cm (favour longer length for T2DM)
o Alimentary limb 100 vs 150 vs 200cm (favour longer length for T2DM)
Agrawal’s technique:
1. JJA with closure of JJA mesenteric window
2. Creation of gastric pouch
3. GJA with leak test
1. JJA with closure of mesenteric window
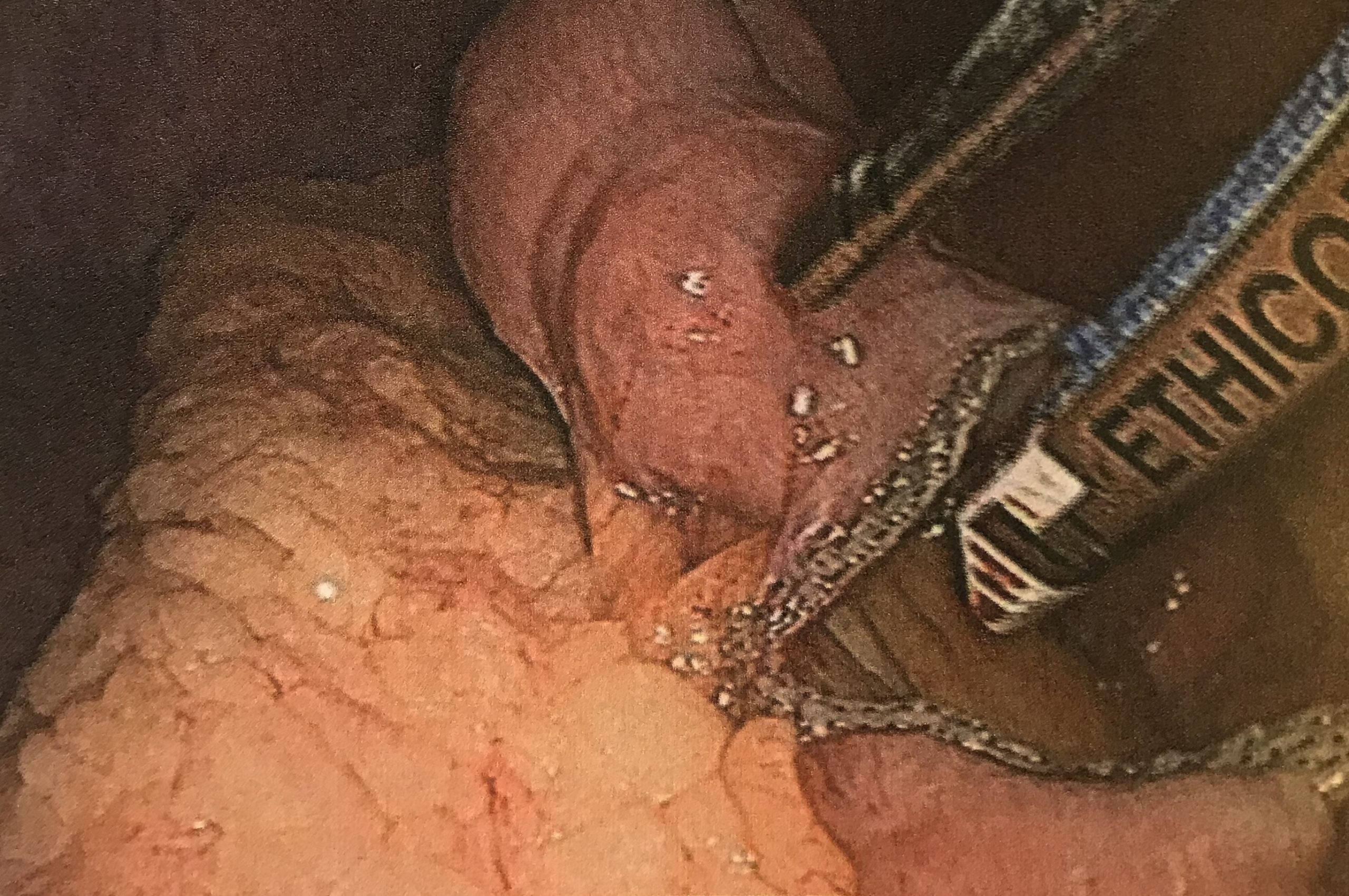
a. Displace omentum to the upper quadrant and identify DJ flexure. Measure BP limb to 25cm and divide with a 45mm 2.5mm (Ethicon white cartridge) linear stapler. Mesentry is divided with a Harmonic. From the distal stapled end, the roux/alimentary limb is measured at 100cm for BMI <40 or 150cm for >40 kg/m2.
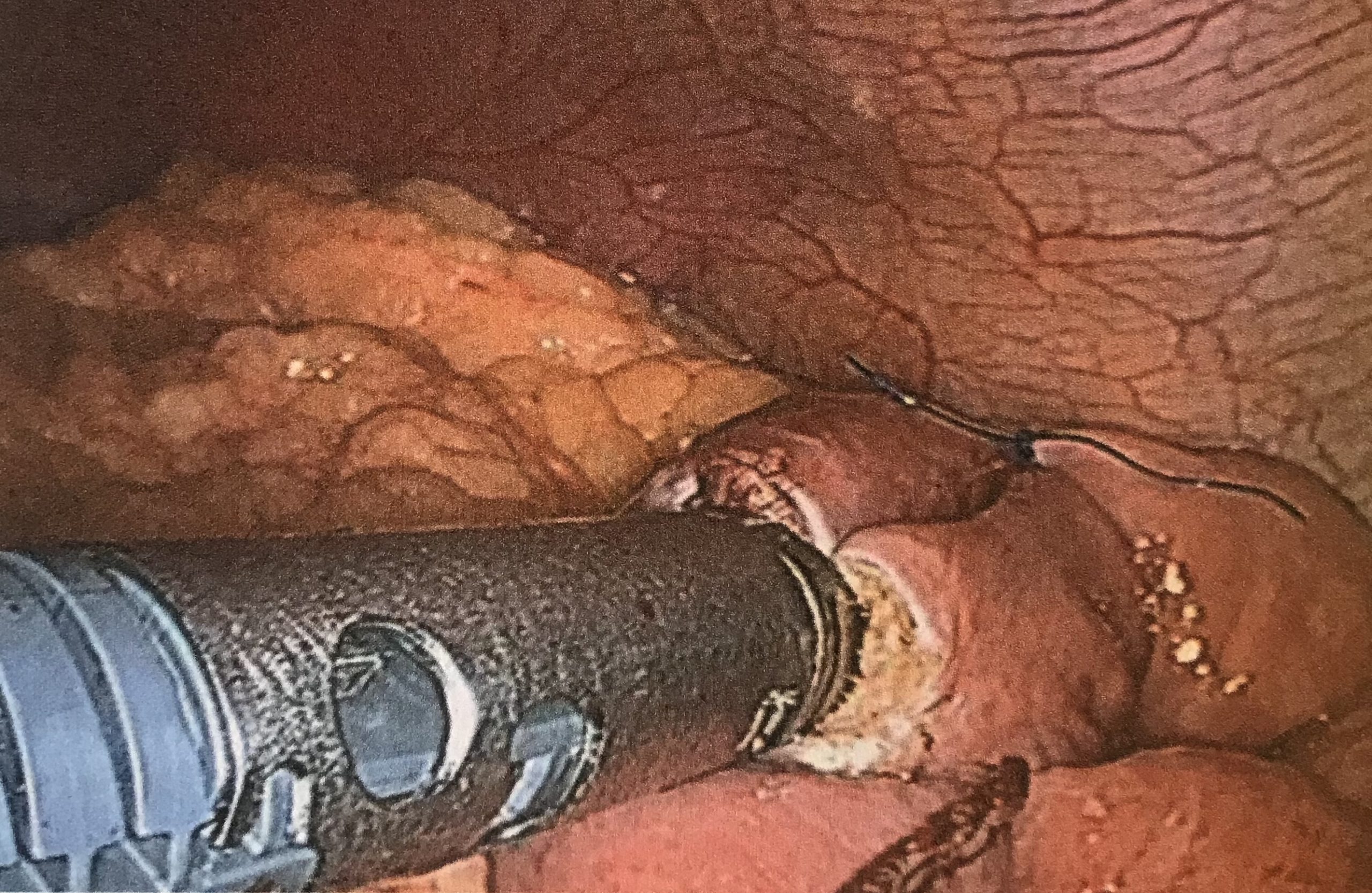
b. The 2 limbs are approximated with a 2-0 monofilament suture at the antimesenteric borders. Enterotomies are performed with the energy device the JJA is formed with one firing of the 45mm white (2.5mm) cartridge. Close enterotomy with 2-0 absorbable monofilament (SA uses 2x monocryl continuous sero-muscular sutures from either end that meet in the middle. A second layer of interrupted sutures can be placed for re-enforcement.
c. Internal hernia defect by the JJA is closed using a continuous purse-string non-absorbable braided suture (Ethibond) The omentum is then split cranially using the harmonic.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2. Gastric Pouch formation
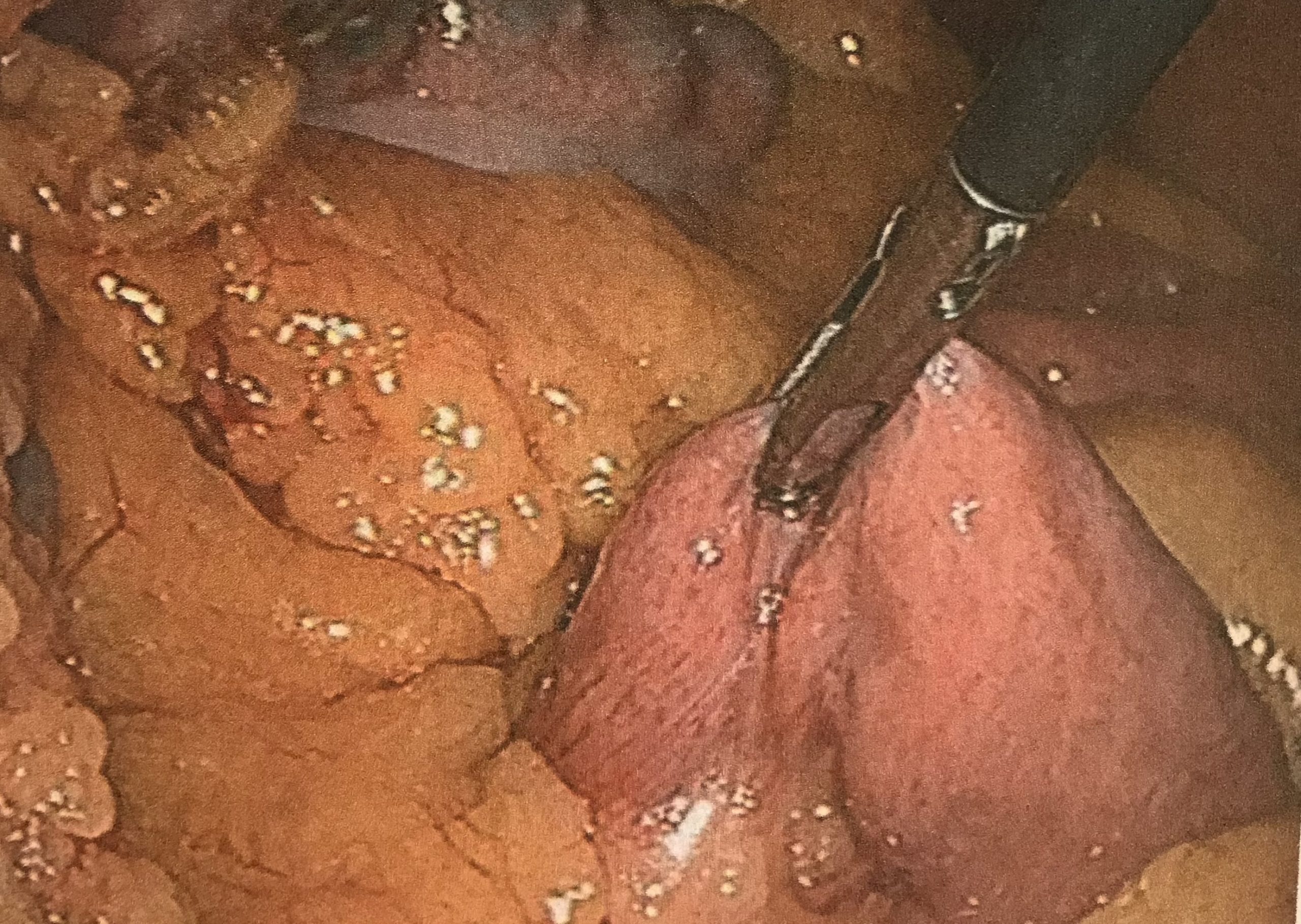
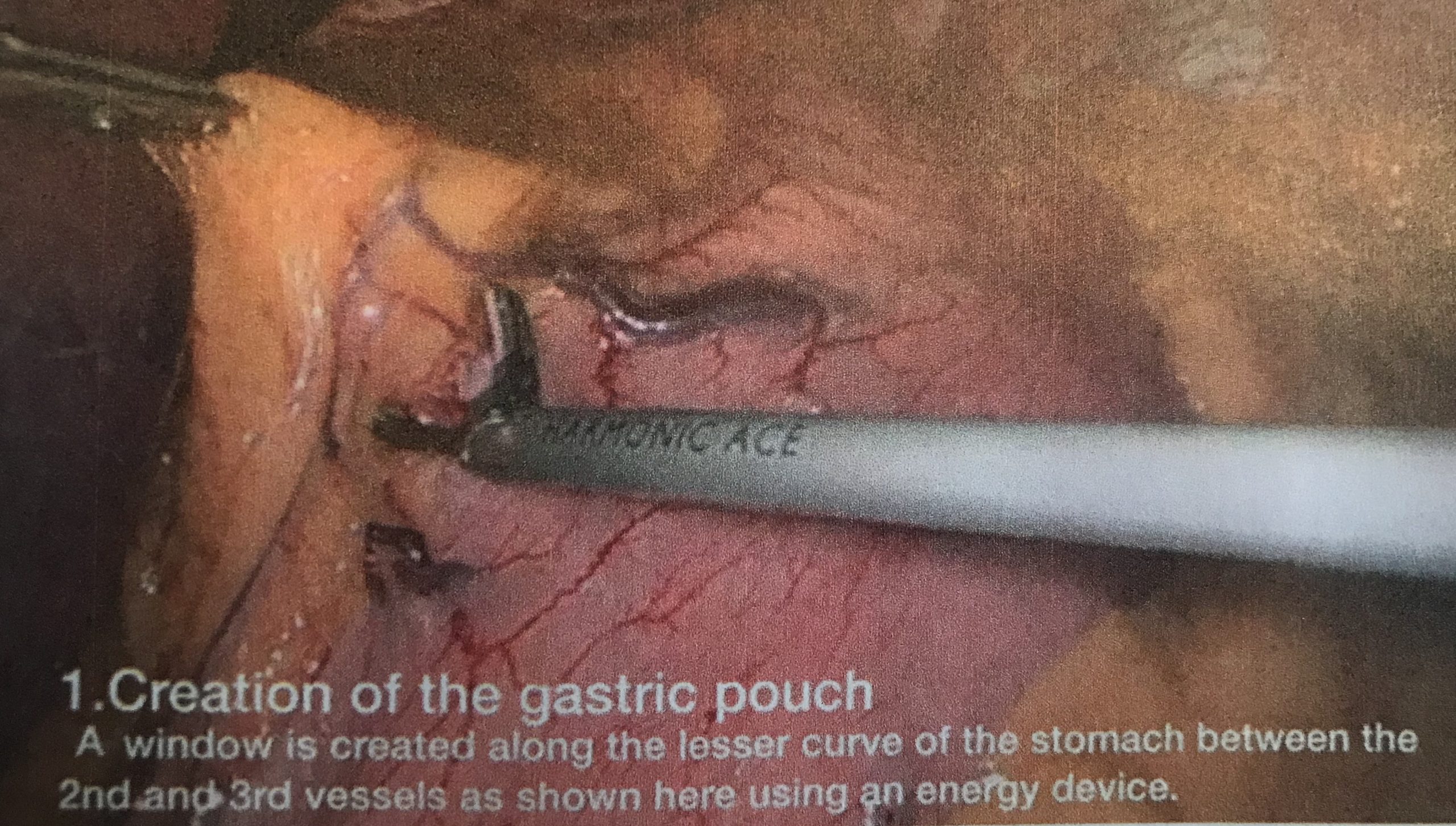
a. Place liver retractor. Create a window in the lesser curve just on the perigastric border between the 2nd and 3rd gastric vessels. Perform blunt + energy device dissection along the posterior gastric wall until the lesser sac is reached.
b. A lesser-curve based pouch is created with firings of a 45mm 3.5mm (Ethicon Blue cartridge) linear stapler in a reverse-L shape. Remove the orogastric tube prior to any firings and position the first firing horizontal to the lesser curve. After this is done, the tube can be replaced into the pouch. The rest of the firings are made caudally. adjacent to the orogastric tube towards angle of His.
c. The volume of pouch should be no more than 20ml.
3. GJA and leak test
a. Make a gastrotomy at the corner between the horizontal and caudal staple lines (likely the most ischaemic area of pouch). The alimentary limb is bought up to the pouch in an antecolic fashion, an enterotomy is made and GJA made with a single firing of a 45mm 3.5mm (blue) linear stapler. Enterotomy is closed with 2 continuous sero-muscular layers over a 30Fr oro-gastric tube with a 3-0 monofilament absorbable sutures.
b. A leak test is performed with 50-100ml of methylene blue dye via the orogastric tube.
4. Check haemostasis, suction out residual fluid, insert Robinson 20Fr drain in LUQ and remove ports under vision.
{kind=link}
Post-operative:
1. Ensure written up for iv antibiotics, iv fluids, omeprazole, ondansetron, analgesia, saline nebs
2. Sips of water by straw only for first night, 20ml of peppermint water every 6h to reduce abdominal discomfort.
3. Daily enoxparain and TED stockings
4. Remove drain usually within 36 hours and discharge home within 48 hours if obs and bloods are acceptable