“…a duct encountered in the gallbladder fossa is likely to be a small superficial intrahepatic duct and can be ligated safely.” The existence of cholecysto-hepatic ducts (running directly from liver to the middle of the gallbladder is controversial. Nagral S, J Minim Access Surg. 2005 Jun; 1(2): 53–58.
Cystic duct
2-4cm in length in 80% of cases 2-3mm wide if not dilated due to passage of stones
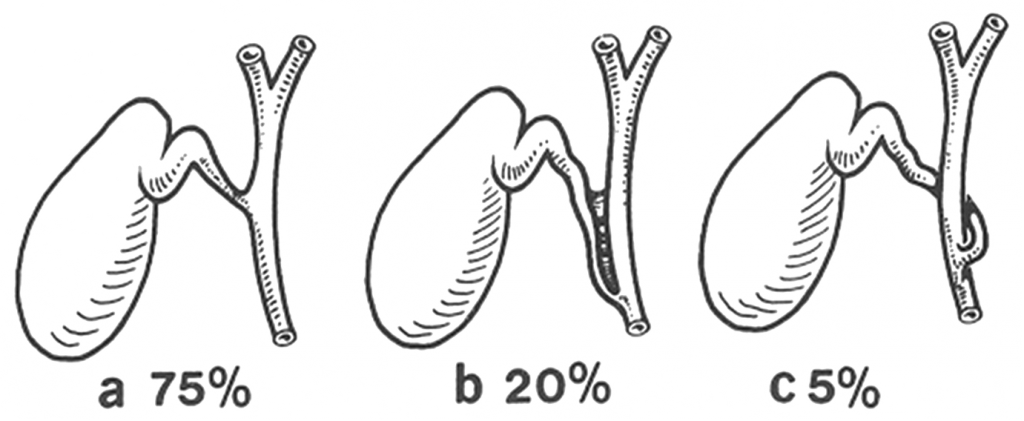
Due to the large variation in how it joins the bile duct, it may not be safe to dissect the junction between cystic duct and bile duct.
Even with long cystic ducts, it’s rare for it to pass behind the duodenum..therefore a structure passing behind the duodenum is likely to be a bile duct.
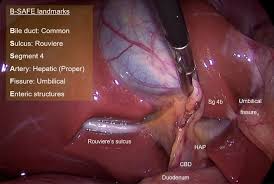
Cystic duct does not have visible vessels travelling on its surface whereas the bile duct does.
Cystic artery and right hepatic artery
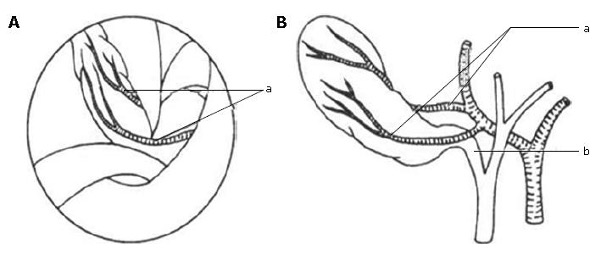
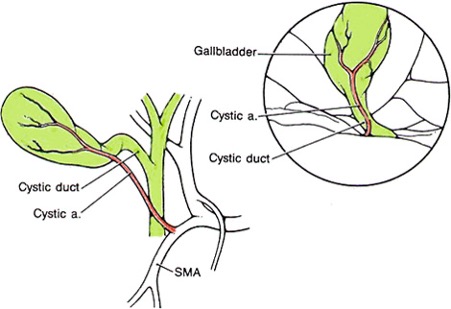
Normally the cystic artery runs through the center of Calot’s triangle but it can be very close to or lower than the cystic duct. Cystic artery usually gives off an anterior and posterior branch as well as small branches to the cystic duct
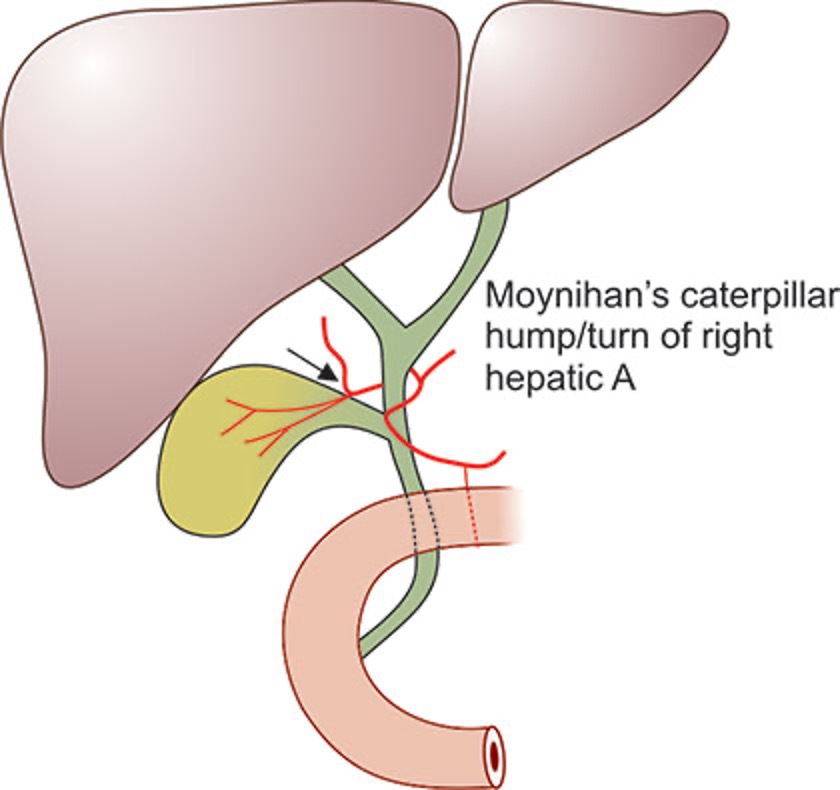
RHA normally runs behind bile duct but it can course very close to the gallbladder.. the ‘caterpillar’ or ‘Moynihan’s’ hump. This can be in as many as 50% of cases and cause a risk of division or tearing during dissection of the cystic artery. Subsequent attempts to stop the bleeding can predispose to biliary injury.
There is a 2-15% incidence of double cystic artery.
There’s also a 2-5% chance that the RHA crosses the bile duct anteriorly.
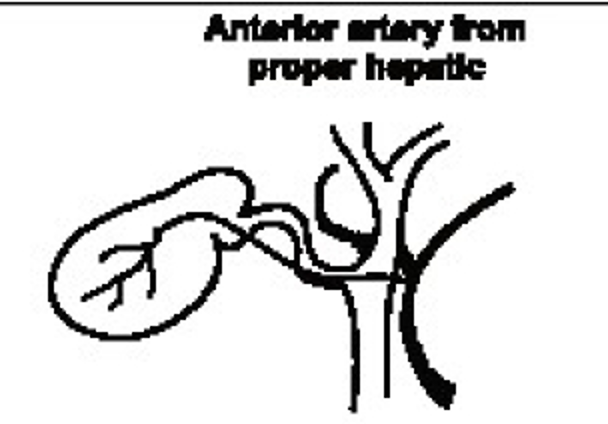
Sometimes the cystic artery arises from the SMA.
If an accessory or replaced RHA arises form the SMA (seen in 15% of individuals) it will travel through Calot’s triangle and give off a short cystic artery.
Accessory and aberrant ducts
Tend to arise from the right hepatic lobe and run through Calot’s triangle to enter the common hepatic duct. They can drain a large part of the right liver. If they are the only drainage for one segment, they are correctly named ‘aberrant’ ducts. Most infact tend to be aberrant and therefore it’s important to preserve them. Incidence of right anterior or right posterior joining the CHA below the confluence is as high as 20%. The size correlates to the amount of liver drained..a rule of thumb is, if it’s larger than 3mm, it should be drained into a Roux loop. Alternatively, a cholangiogram can demonstrate the amount of liver its draining.