Inguinal hernia repair
Consent
Complications of anaestesia
General complications: pain, bleeding, infection, scarring, DVT/PE
Specific complications:
– Swelling at site of hernia, seroma/haematoma (1:10)
– AUR (1:100)
– Injury to organs within hernia
– Chronic pain – mild (1:4), severe (3:100)
– Injury to nerves (<1:10)
– Damage to blood supply to testicle
– Recurrence (if mesh used <2:100)
Recovery
Shouldn’t drive / operate machinery (inc. cooking) / sign legal documents / drink alcohol for 24 hours
Gradually increase walking over next few days
Return to work 2-4 weeks
No heavy lifting for six weeks
Anatomy
- Inguinal ligament runs from the pubic tubercle to the Anterior Superior Iliac Spine (ASIS)
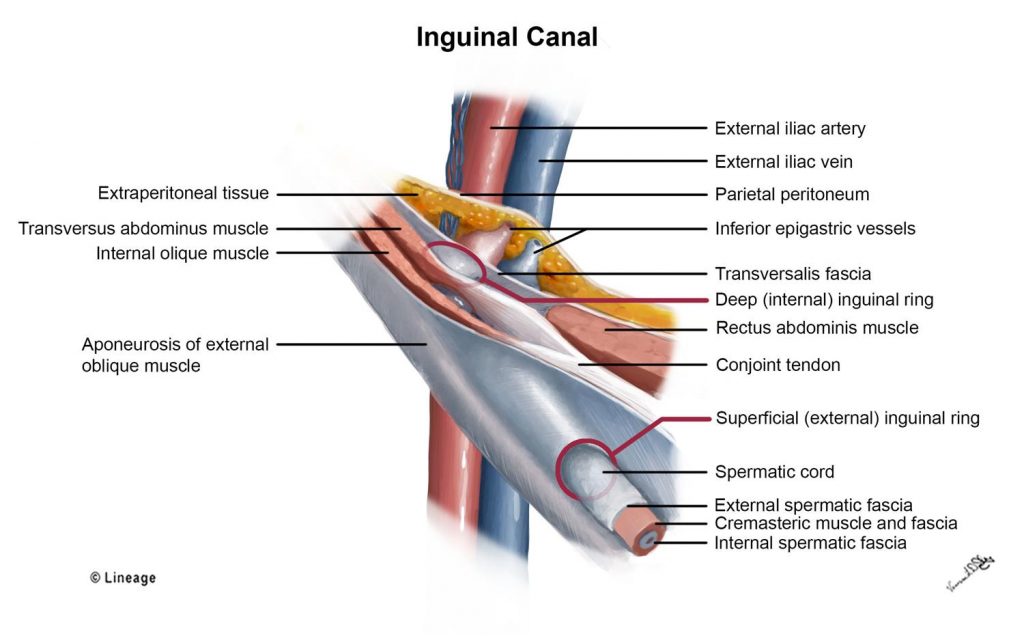
- Deep inguinal ring is found at midpoint of the inguinal ligament
- Superficial inguinal ring is just superior to the pubic tubercle.
- The inguinal canal is approximately 4cm long
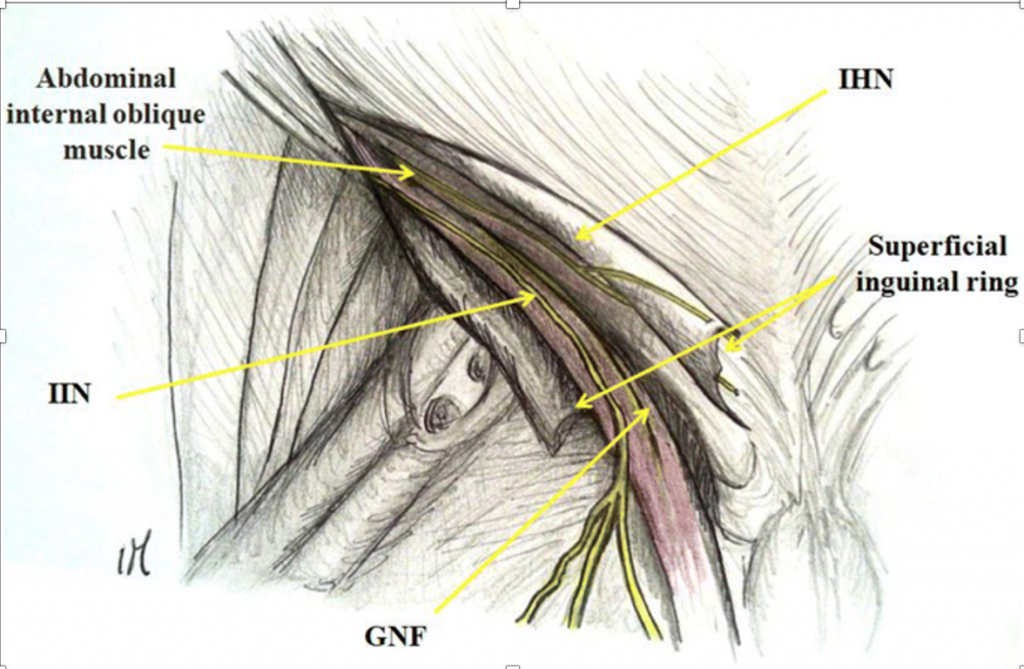
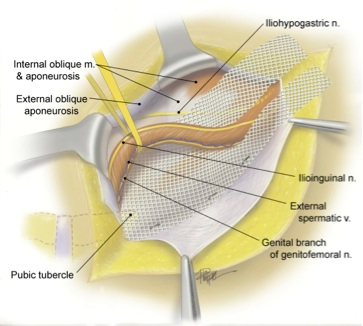
- MALES: contents are spermatic cord (vas deferens, spermatic and cremasteric arteries and veins, genital branch of the GFN), IIN and IHN
- FEMALES: contents are the round ligament of the uterus which attaches to the labia majora, genital branch of the GFN, IIN and IHN
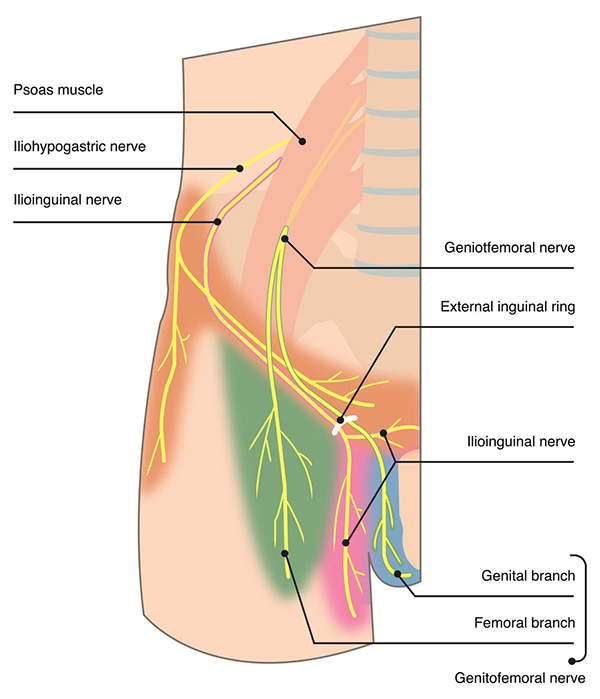
- Nerves:
- IIN, IHN and GFN are terminal branches of the lumbar plexus
- The (anterior branch of) iliohypogastric nerve runs between transversus and internal oblique, pierces the internal oblique approximately 2 cm medial to the ASIS to run within the inguinal canal and then exits by piercing the external oblique approximately 3cm above the superficial ring
- Provides sensation to the medial suprapubic skin
- The (anterior branch of) iliohypogastric nerve runs between transversus and internal oblique, pierces the internal oblique approximately 2 cm medial to the ASIS to run within the inguinal canal and then exits by piercing the external oblique approximately 3cm above the superficial ring
- The ilioinguinal nerve emerges into the abdominal wall (transversus) approximately 2 cm inferior and 3 cm medial to the ASIS to run along the spermatic cord and exit with it through the superficial ring.
- In males, supplies proximal medial skin of the thigh, inguinal crease, upper scrotum and lateral base of the penis
- In females, it innervates the skin covering medial thigh, mons pubis and labia majora.
- There’s huge variability with IIN, with 43% of patients having an aberrant course (eg. reconnection with IHN, duplication, posterior to spermatic cord)
- The ilioinguinal nerve emerges into the abdominal wall (transversus) approximately 2 cm inferior and 3 cm medial to the ASIS to run along the spermatic cord and exit with it through the superficial ring.
- The genitofemoral nerve splits just above the inguinal ligament into the genital branch (passes through the transversalis to enter the spermatic cord) and the femoral branch (passes in front of the femoral artery). The genital branch passes over the external iliac artery and traverse the deep inguinal ring to join the cord structures/round ligament to run within the canal.
- In males, provides motor innervation to creamasters and skin of upper scrotum
- In females, it innervates the mons pubis and labia majora.
- The most variable of the three nerves but the inguinal canal portion is fairly consistent (97% identification within cord)
- The genitofemoral nerve splits just above the inguinal ligament into the genital branch (passes through the transversalis to enter the spermatic cord) and the femoral branch (passes in front of the femoral artery). The genital branch passes over the external iliac artery and traverse the deep inguinal ring to join the cord structures/round ligament to run within the canal.
- The Lateral Femoral Cutaneous nerve can genitofemoral trunk traverse the pre-peritoneal plane and can be injured in posterior repairs
- Passes behind or through inguinal ligament, approximately 1cm medial to the ASIS (halfway between ASIS and femoral artery
- Anterior branch supplies anterior and lateral thigh to the level fo the knee
- Posterior supplies the lateral thigh from greater trochanter to mid-thigh
- The Lateral Femoral Cutaneous nerve can genitofemoral trunk traverse the pre-peritoneal plane and can be injured in posterior repairs
- Obturator nerve and femoral nerve can also be injured in their preperitoneal plane during laparoscopic repair
- Coverings of the spermatic cord:
- External spermatic fascia (derived from external oblique)
- Cremasteric fascia (derived from internal oblique and transversus fascia/muscle)
- Internal spermatic fascia (derived from the trasversalis fascia)